


ABA SOAP notes simplified: How-to, expert advice, and templates

Inside this article:

All healthcare fields rely on SOAP notes, and ABA is no exception. The impression you make in your notes matters to patient outcomes. Delve into our guide to find a detailed description of ABA SOAP notes, expert tips, and three completed examples.

[fs-toc-omit]What Are ABA SOAP Notes?
ABA SOAP notes refer to a common notetaking template that applied behavior analysis (ABA) providers use to describe a session with a client. ABA SOAP notes help different clinicians communicate patient progress in a standardized way. The notes also serve as proof for insurance claims.
The acronym SOAP stands for the four sections included in the notes: Subjective, Objective, Assessment, and Plan. Together, SOAP notes provide a systematic assessment of a client’s progress and interventions. SOAP notes provide a concise, written history of what a therapist observed and can be useful for professional communication to validate insurance claims. Also, the structure of SOAP notes allows professionals to identify and track client progress. Insurance companies and litigation professionals look to SOAP notes to substantiate billing requests and treatments.
SOAP notes originated in the late 1960s when Dr. Lawrence Weed became frustrated with the lack of standardized documentation in the medical field. Dr. Weed saw the need to communicate diagnoses and opinions about patients with complex presentations requiring diverse doctors’ care. To solve this issue, Dr. Weed developed the Problem-Oriented Medical Record (POMR) system, which eventually evolved into SOAP notes.
Many healthcare fields have adopted SOAP notes as the standard format for professionals to detail an interaction with a client to another professional in a structured way. Generally, SOAP notes represent a standard way for healthcare professionals to communicate with one another to assess, diagnose, and treat a patient.
Finally, consider that SOAP notes serve as the documentation between you and the other professionals in your client’s life – including your boss, your client’s doctor, and insurance providers. Some of these professionals will determine how long your relationship is with your client, and others will use your notes to inform their treatment plans with your client. Taking precise SOAP notes that provide excellent clinical rationale elevates your therapy in the eyes of other professionals.
In the ABA setting, SOAP notes describe any session conducted by a Board-Certified Behavior Analyst (BCBA) or a Registered Behavior Technician (RBT) with a client. SOAP notes form an important part of ABA data collection, alongside session notes. But SOAP notes and session notes differ in subtle but important ways.
According to Taylor Gaines, MS, BCBA, “session notes are more structured than SOAP notes. They are used to track data daily on the treatment plans. We use session notes to track data daily on the treatment plan, including any notes on behavioral intervention plans, preference assessment data, and required materials to run that session. On the other hand, SOAP notes only capture specific information during a session and don’t include as much data. SOAP notes focus on subjective data, an analysis of the session, and future planning for the client’s therapy.”
Key Takeaways:
- SOAP notes serve as written proof for insurance claims and provide a systematic way for healthcare professionals to communicate.
- Insurance companies do not maintain a universal SOAP note standard.
- Writing an effective SOAP note requires practice and a thorough understanding of each component.
- The best SOAP notes are concise, objective, and only include relevant information.
- Digital SOAP notes allow clinicians to take detailed notes throughout a session, saving time and energy.
[fs-toc-omit]ABA SOAP Notes Components
SOAP notes contain four sections. The subjective section includes relevant client opinions. The objective section contains measurable data. The assessment section provides analysis and diagnosis. Finally, the plan section describes what the therapist will do in the next session.
The four sections in SOAP – subjective, objective, assessment, and plan – take the reader and writer through various queries that, together, make up a holistic perspective of the session and progress. Each section leads logically into the next. The subjective section contains information about the problem from a client’s perspective, and the objective section contains measurable observations from the BCBA. The BCBA analyzes the information in these portions in the assessment section to make a professional interpretation or diagnosis. Then, the BCBA notes treatment direction in the plan section.
Here’s a summary of the four components of SOAP notes.
The Subjective (S) Section of SOAP Notes
The Subjective (S) component documents information directly from a patient or someone close to the patient relevant to the patient’s condition or status. This information represents a patient’s subjective description of their condition and includes information that is not measurable.
The subjective component should read like a narrative of a patient’s self-report of their status. Be sure to use quotation marks when you directly quote a patient.
Generally, the subjective portion will be three or four sentences, but it might be longer if social history and medications apply. This section typically covers:
- Current condition and chief complaint
- Level of function
- Symptoms
- Direct quotes from the patient
- If directly relevant, the patient’s social history, including employment status and pertinent family information
- If directly relevant, current medication and allergies
- Any information that might have affected the patient’s session, such as if they were sick or inattentive.
Avoid the following types of content:
- Including opinionated language about a patient’s self-report. For example, avoid saying, “Bill is overwhelmed by stress from work and should take a week off.” This sentence reads as an opinion unless Bill states he wants to take a week off work. In that case, the note should be rewritten as a direct quote from Bill.
- Documenting superfluous information about the patient’s condition or session, like the patient’s opinion of their previous BCBA.
The Objective (O) Section of SOAP Notes
This section reports objective information about the patient that can be measured and is entirely factual. For example, suppose a BCBA performs any assessments or interventions, like discrete trial training (DTT) or picture exchange communication system (PECS). In that case, the therapist can include the results in table form or write them out.
The objective statement helps a BCBA assess the progress toward goals and detail when new symptoms begin to manifest.
You should include information about the following:
- General appearance and affect
- Observations on the physical and psychological mannerisms of the patient
- Client’s engagement level and willingness to participate
- Measurements, if applicable (e.g., heart rate, weight, PELS scores, etc.)
- You can include tables when reporting objective results from a task
Avoid the following types of content:
- Vague statements that could not have been measured
- Personal judgments (avoid using language like “seems”)
- The use of language with negative connotations (annoying, drunk, etc.) For example: “Bill doesn’t value our sessions because he seemed distracted and ignored some of my questions.”
The Assessment (A) Section of SOAP Notes
Under the assessment section, the BCBA synthesizes the information in the objective and subjective sections to note progress, regression, or a plateau in the client’s progress. Think of the assessment section as your chance to answer “why” certain observations or client performances happened in the “O” section. Then, if the BCBA makes a diagnosis, adequate data in the O and S sections should support the claim.
This section should be the bulk of the SOAP note and is the BCBA’s chance to identify themes or patterns and update any clinical criteria related to a behavioral assessment. When other colleagues or outside reviewers review your SOAP notes, they typically will read the assessment section first.
Include the following types of content:
- Differential diagnoses for any new symptoms
- Changes from the last session
- Client response to any intervention – insurance providers may look here for evidence that the interventions are working
- Possible reasons and explanations
Avoid the following content:
- Repeating information already provided in the objective section
- Speculation about conditions or issues that you did not include in the objective section.
The Plan (P) Section of SOAP Notes
In the plan section, the BCBA will detail what interventions the patient needs and outline the next course of action in the treatment plan. The plan section should include goals of therapy and any medications.
Include the following types of content:
- Focus on the future and include the next steps for an upcoming session
- Note any progression or regression the client made in the session
- Include short-term goals and interventions
- Reflect on which strategies worked and didn’t work during the session
Avoid including:
- Lofty goals that can’t be accomplished by the next session
- Re-summarizing the overall diagnosis or treatment instead of focusing on the goals for the next session
Learn more about ABA Data Collection: Method, Tips, & Tech
[fs-toc-omit]Why Are ABA SOAP Notes Important?
SOAP notes offer proof of what a BCBA did and observed in a session. The notes also allow professionals to communicate effectively about a patient. SOAP notes can establish credibility when receiving insurance reimbursements or during an audit.
Precise documentation is integral to ABA and patient care. Clients rarely see only one therapist or medical professional but must coordinate care with many. Other professionals count on you to properly document your interactions with your patient. Failing to do so can lead to misleading or confusing information, negatively impacting the patient’s overall medical care. Finally, BCBAs commonly look to older SOAP notes when asking where another BCBA left off. The structured nature of SOAP notes means they can serve as a useful index to look up specific information quickly.
Insurance and auditing agencies also have adopted SOAP notes to corroborate treatment claims and assess work systematically. Proper SOAP notes will show insurance providers that you are providing a skilled service that benefits your patients.
Here’s a list of SOAP note benefits:
- Helps keep track of client progress
- Aids a therapist in assessing information to create a treatment plan
- Improves quality of care
- Enables medical professionals to share information
- Communicates essential information with insurance companies
- Provides an easy way to reference previous sessions
Helps establish credibility with other medical professionals
How to Write ABA SOAP Notes
To write effective ABA SOAP notes, include a section on each of the four components with relevant, succinct information. Include critical information and use a formal, neutral tone. Don’t repeat information from one section in another.
Gaines notes that “all SOAP notes should include the date, time, location, who was present, the provider’s name, the client’s name, and the client’s date of birth. Some insurance companies require program modification information to be added to the SOAP notes. In addition, some insurance companies require notes to be written in the third person, and some require therapist names in each section.”
Sherry Cyrus, Medical Billing Manager at Plutus Health Inc. echoes these comments and adds that “ABA SOAP notes should have a corresponding assessment and treatment plan. The treatment plan is developed as part of the assessment and drives the provision of ABA and treatment services. It must contain, at a minimum, the following elements, in addition to any state-required components:”
- The patient’s name is documented on each page of the record
- The date of service is documented on each page of the record
- Type of service (e.g., diagnostic assessment, individual, family, group psychotherapy)
- Start and end times
- Problem statement (including diagnosis)
- Support for medical necessity services rendered including therapeutic interventions
- Person-centered detail such as behavior description or quotes
- Patient observation
- Rationale for exposure assessments and interventions including attention to safety measures
- Summary of progress or lack thereof toward identified goals; lack of progress should result in a change in plan or a new plan of care (this should include, for each treatment goal, baseline measurements, progress to date and anticipated timeline for achievement based on both the initial assessment and subsequent interim assessments over the duration of the intervention)
- Protocols used in treatment and how they tie back to treatment plan
- Protocol modification should be documented as a distinct and specific activity
- Coordination of treatment with other healthcare providers and, when applicable, service organizations outside of healthcare such as schools or vocational rehabilitation should be documented
According to Cyrus, medical billing manager at Plutus Inc., insurance companies “follow Centers for Medicare & Medicaid Services (CMS) guidelines which requires that medical record documentation should be legible, signed (including licensure and/or certification), dated, and must contain certain information in addition to any state required components. Providers are required to maintain individual medical records that are in conformance with standard professional practice. “
Overall, Cyrus adds, “insurance companies require providers to maintain medical records in a manner that is current, detailed, organized, and permits effective and confidential patient care and quality review. Providers are also required to maintain individual medical records that are in conformance with standard professional practice.”
Unfortunately, insurance companies can differ in the fine details of their ABA SOAP note requirements. As a result, BCBAs must be well-versed in the requirements for all their insurance partners. Otherwise, insurance companies may deny payments based on incomplete SOAP rules. Cyrus cautions that “improper notes can lead to inaccurate billing, which may result in an audit.”
Every BCBA and ABA business leader must take the time to navigate their specific providers’ regulations to create a systematic workflow and SOAP template.
Download Your ABA SOAP Note Template
Use this template to create clear, consistent, and customizable ABA SOAP notes
Examples of Effective ABA SOAP Notes
We provide three examples of effective ABA SOAP notes alongside our comprehensive template. Note that every example differs in patient behavior and prognosis. But every SOAP note includes the same type of information in each section.
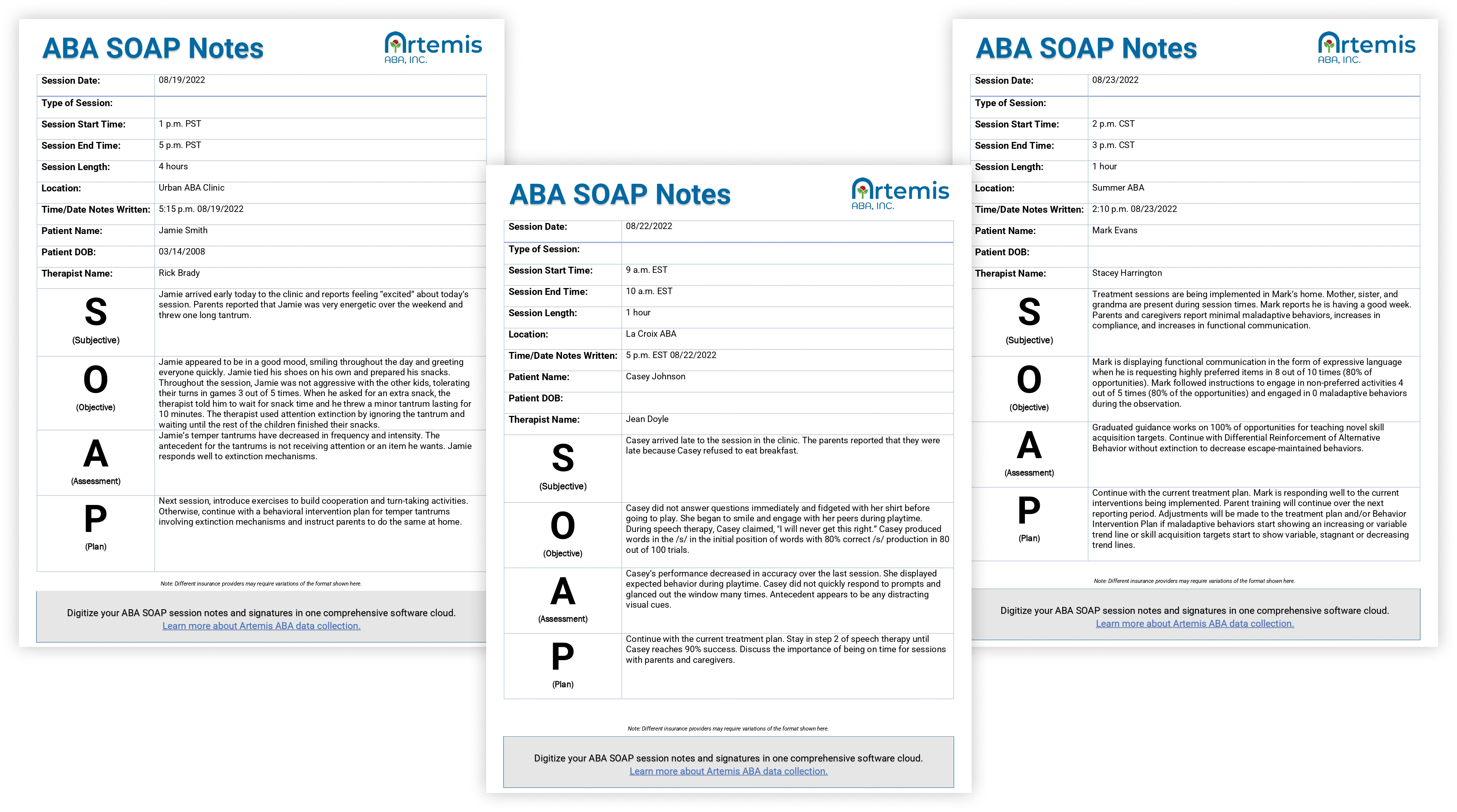
Download our ABA SOAP notes examples for reference
Mistakes to Avoid When Writing ABA SOAP Notes
Writing a good ABA SOAP note takes time and practice. Most BCBAs will make some common mistakes as they learn. These include using informal language, writing in the present tense, and using judgmental language.
Gaines, BCBA, points out that “behavior is what we do, not what we don’t do. Avoid using negatives when writing notes. For example, “Jon did not engage in functional communication” is much less informative than “Jon engaged in three instances of functional communication over the last hour.”
Here’s a list of common mistakes to avoid when writing SOAP notes and options for what to do:
- Misattributing statements
When your client tells you he is in a good mood, don’t write “the client seemed to be in a good mood,” but rather “the client stated he was in a good mood.” - Using judgmental and opinionated language that conveys personal, rather than professional, opinion
These words include obnoxious, annoying, normal, drunk, manipulative, and others. Instead of using these and related terms, record the details of what you observe. For example, rather than writing “the learner could not even say his mother’s name,” try to note what actually happened – “the learner verbalized his mother’s name after the BCBA prompted him to do so twice.” - Providing subjective statements without evidence
Don’t write, “Steve was frustrated.” Instead, note the actions that led you to form that belief. For example: “Steve sighed audibly multiple times through the session and slammed his fist on the table when he answered questions incorrectly.” - Using words like “seems” or appears” that change the interpretation of objective observations
For example, the sentence “Jill seems to be angry” contains some ambiguity, whereas “Jill yelled and threw her shoe at the BCBA” describes a factual incident. - Using idioms and informal language
Remember that other colleagues and insurance providers will use SOAP notes to assess your work. Maintain a formal voice throughout your SOAP notes. For example, don’t write that “Cindy had a blast.” Instead, “Cindy smiled and laughed during the games session.”
[fs-toc-omit]Best Practices for ABA SOAP Notes
To improve your SOAP notes, follow some standard best practices. For example, use clear language, avoid jargon, and always use the active voice. Also, follow standard procedures to improve the readability of your notes, like using headings or tables.
Here are some common best practices that will add an extra air of professionalism to your documentation:
- Be concise and clear with your notes: The systematic format of SOAP notes pairs well with concise, clear language. Don’t include flowery language that bogs down the point of the sentence.
- Use the active voice: Avoid language that makes you seem like a passive observer. Remember, you are a skilled clinician and provide an important service. Use active verbs like “assess,” “train,” “teach,” “provide,” etc. For example, instead of writing that “the RBT observed the client perform two trials,” consider writing “the RBT taught the client how to perform two trials and then assessed his performance.”
- Use headings to improve readability: SOAP notes serve as a helpful index for other health professionals to quickly retrieve information. Use headings for ease of readability, especially for longer SOAP notes that describe a complex or lengthy session.
- If you make an error, do not alter the note: Instead, systematically note the error, and write the correction, along with your initials and the time of corrections. Be sure the mistake is still readable, showing that you are trying to clarify the issue, not hide it.
- Include bulleted lists and tables when appropriate: Tables work well to communicate objective results of assessment tests and help the reader locate important information quickly.
- Only use standard abbreviations: Standard abbreviations that BCBAs and other healthcare professionals understand can help make your SOAP notes succinct. On the other hand, using complex or uncommon abbreviations will confuse the reader.
- Proofread: We all make mistakes, but simple typos and common grammatical errors will appear unprofessional. So, budget an extra few minutes for proofreading your writing.
Use an ABA SOAP note template

An ABA SOAP note template can help you and your colleagues expedite the process and improve standardization. A template also reduces ambiguity between BCBAs who may have different personal styles. Clear communication will translate to better patient care.
Get started with our ABA SOAP notes template.
Expert Tips for ABA SOAP Notes
Sharpen your SOAP notes with expert tips straight from ABA professionals. ABA experts know the practice of writing SOAP notes differs from theory. Learn which in-clinic routines cultivate effective SOAP notes and which habits make them seem like a chore.
To master SOAP notes, follow these expert tips straight from Gaines, who has worked in ABA since 2005.
- “If you cannot write your notes immediately after the session, make sure to write them within 24 hours.
- “Take good notes during the session so you can organize and transcribe later.”
- “Be thorough but not wordy. Stick to the basics and give important information.”
- “Make sure to include notes on your plan of action so you can follow through with all changes to treatment plans and behavior plans when applicable.”
- “Educate yourself on insurance requirements and generalize them across all notes – the more identifying information the better.”
Alongside these tips, Cyrus, Medical Billing Manager at Plutus Inc., adds the following:
- “When in doubt, follow guidance from the Centers for Medicare & Medicaid Services (CMS).”
- “Use a practice management solution that’s specific for ABA that utilizes data collection. This practice will allow detailed and customized notes and treatment plans to be created that will ultimately benefit the client.”
Digital ABA SOAP Notes Improve Customer and Staff Experience
Digital ABA SOAP notes streamline the entire process of ABA documentation. Capture notes throughout the session and have instant access to history and treatment data. These features translate to more accurate notes, less stress for providers, and improved patient care.
Digital (or electronic) ABA soap notes have become the gold standard in healthcare documentation. Instead of manually transcribing notes at the end of a session, digital SOAP note platforms allow you to make quick notes in the moment of observation – when your thoughts will be most accurate and helpful. Many programs compile these notes into a preliminary SOAP note. In addition, some will allow you to dictate notes straight into the program, a handy feature for BCBAs who often have their hands tied up!
For Gaines, digital SOAP notes have completely changed client care. Speaking about her own team of ABA professionals, Gaines points out that “taking notes digitally allows the entire team to have access to the client’s progress and any changes to the treatment plan immediately and daily. With this capability, we can better serve our clients as a team and, because everyone is on the same page with the client’s treatment plan, make sure that the client is receiving the most effective treatment.”
Digital SOAP notes represent just one of the facets of a digital ABA practice that build resiliency and efficiency into an ABA practice. Alongside automated billing authorizations, electronic session notes, and session management tools, you’ll save hours of time and energy. These tools are indispensable to everyone, from seasoned ABA professionals to those looking to start a new ABA practice.
[fs-toc-omit]How Artemis Improves ABA Session Notes and Data Collection
Artemis integrates SOAP and session notes into your day-to-day duties with a single cloud-based solution. Use the latest AI technology and transform session notes from a tedious task to an empowering tool for patient care.
The Artemis ABA practice management software supports any data collection with flexible, comprehensive software. For example, SOAP notes may be a longstanding system, but that doesn’t mean you still have to take your notes manually. With real-time ABA session notetaking capabilities, you won’t have to pause a session or hope you remember the important details for the end of the day. Instead, jot down a quick note when the moment happens directly into the Artemis Session Management platform.
Gaines, BCBA, knows firsthand how difficult it can be to juggle meaningful notetaking with ABA sessions. “Typical therapy sessions feature a lot of activities, behaviors, and environmental changes,” Gaines says. “Artemis allows you to take real-time notes throughout the session, which is incredibly helpful. With Artemis, you can take notes throughout the session and compile them together at the end. This way, you won’t forget information and have a clear picture of what occurred during the session.”
The experts at Artemis know that no two ABA businesses are the same. So, they designed the Artemis platform to support various data types and ABA specialties. Finally, Artemis doesn’t rely on integrations, which can be unreliable and cause you to lose time, resources, and valuable patient data. Instead, their software digitizes all elements of an ABA practice – from data collection to insurance compliance – to provide a true 360-degree view of an entire business.
Leave the business workflow to Artemis so you can direct all of your energy to what brought you to ABA in the first place – your patients.
Schedule Your Walkthrough

Frequently Asked Questions
What are ABA SOAP notes?

ABA SOAP notes are structured clinical notes that document session details using Subjective, Objective, Assessment, and Plan sections.
Why are SOAP notes important in ABA therapy?
SOAP notes ensure that sessions are documented clearly to support clinical continuity, supervision, compliance, and insurance requirements.
What goes into the Subjective and Objective sections of ABA SOAP notes?
The Subjective section captures observations and reports from caregivers or therapists, while the Objective section records measurable behavior data from the session.
What is included in the Assessment and Plan sections of ABA SOAP notes?
The Assessment summarizes client progress and clinical interpretation, and the Plan outlines next steps, program updates, or focus areas for future sessions.
What are common mistakes in ABA SOAP note documentation?
Common mistakes include vague language, missing data, late entries, and notes that do not align with billed services or treatment goals.
How does Artemis ABA support ABA SOAP notes?
Artemis ABA streamlines SOAP note creation with structured templates, linked session data, and timely completion tracking to keep teams compliant and audit-ready.
Monday to Friday, 7 AM – 7 PM CST.
If you're reaching out outside these hours, please submit a support ticket—our team will respond as soon as possible.


%201.webp)


