


How to Use Component Analysis in ABA: Methods, Steps and Template


Inside this article:

Master ABA component analysis to isolate active components in treatment packages. This guide provides a step-by-step framework for add-in and drop-out methods, research examples, and a graphing template to simplify data analysis and optimize treatment.
Quick summary:
Component analysis in ABA helps clinicians identify which parts of an intervention drive behavior change. Practitioners use add-in methods to build or improve interventions and drop-out methods to simplify treatments that already work. Strong analyses require stable baselines, clear conditions, and changes to one variable at a time. Clinicians can apply reversal, alternating, or multiple baseline designs depending on the learner, behavior, and goal. This article explains the steps, examples, graphing process, and decision points for choosing the right component analysis method. It includes a component analysis readiness checklist and a graph template.
[fs-toc-omit]How component analysis works in ABA
ABA clinicians use component analysis to identify which parts of an intervention drive behavior change. Instead of treating an intervention as a single unit, they break it into components and evaluate how each affects behavior. This process helps them identify what is necessary to create more effective and efficient interventions.
Component analysis is a standard procedure in ABA and is included in foundational texts such as Applied Behavior Analysis by Cooper, Heron, and Heward. It’s also a required skill in the BCBA Task List, a summary of the core knowledge a BCBA needs, published by the Behavior Analyst Certification Board (BACB).
To describe a component analysis, clinicians use specific terminology. A treatment package is an intervention a practitioner designs to achieve a goal, such as reducing a behavior, increasing a skill, or teaching a new response. A component is a single, independent part of that package. Clinicians can implement and measure each component separately, even though they often combine them. An active component is one that meaningfully contributes to the outcome and is necessary or sufficient to prompt behavioral change. Treatment packages are usually synonymous with, or part of, an ABA behavioral intervention plan.
Although treatment packages often produce strong results, they can become unnecessarily complex or resource-intensive. Component analysis helps clinicians determine which elements actually matter and answers a key question: Which parts of this treatment actually drive behavior change?
For example, a treatment package designed to reduce problem behavior might include differential reinforcement, prompting, and extinction. Each represents a distinct intervention that can influence behavior on its own or in combination with others. A component analysis might reveal that prompting is not an active component, leading the clinician to streamline the intervention and use only reinforcement and extinction.
[fs-toc-omit]Technical requirements of ABA component analysis
An ABA component analysis tests how each part of an intervention affects behavior. To gain experimental control and show that a component causes change, clinicians need a stable baseline, clear conditions, and can only change one variable at a time.
Dr. April Haas, BCBA-D, LBA-TX notes that while component analysis is a key methodology in ABA, the terminology and formal designs are more commonly used in research settings.

“Clinical decision-making is always grounded in scientific principles, but clinicians often place more emphasis on improving outcomes for learners than on maintaining strict experimental control,” Haas says. “For example, if we see that a component is working very well to create positive change, we may not continue with a full experimental design.”
She also highlights a difference in how practitioners talk about these processes in practice. “We typically say ‘intervention’ or ‘BIP’ in practice, not ‘treatment package’ or ‘active component.”
In contrast, research settings place a stronger emphasis on experimental control, says Dr. Kristi Morin, PhD, BCBA-D. She is the founder and owner of ABA Exam Prep Reimagined, where she helps people struggling to pass the BCBA exam gain the knowledge, skills, and confidence they need to succeed.

“Component analysis is about identifying which parts of a package are responsible for behavior change,” Morin explains. “If you want to rule out alternative explanations, you need strong experimental control. That means establishing a stable baseline, clearly defining conditions, setting criteria for switching phases, and isolating one variable at a time while keeping others constant. And, most importantly, creating a design where you have at least three opportunities to determine if the changing the component has an effect on behavior.”
Here are the key prerequisites that allow clinicians to isolate individual components, evaluate their effects, and determine which parts of an intervention drive behavior change:
- Defined and complete treatment package: Clinicians must clearly define all parts of the intervention before testing them. A component analysis works only if you know exactly what you’re evaluating.
- Isolated variables: Each component must function as an independent variable. The clinician changes only one component at a time so they can attribute behavior change (the dependent variable) to that specific element.
- Baseline stability: The target behavior should be stable and predictable before introducing or removing components. This ensures that later changes reflect the intervention rather than natural variability.
- Steady state responding: Within each condition, behavior should reach a consistent level, or exhibit “steady state responding,” before the practitioner changes phases and either adds or removes a component.
“You need to decide ahead of time what level of performance you’re aiming for and how many sessions you’ll run before making a change,” explains Morin. “In research, that typically means collecting at least three sessions of stable data within each phase before switching conditions.”
Primary methods for ABA component analysis
Clinicians use two main methods to conduct a component analysis: add-in and drop-out. In an add-in method, clinicians introduce components one at a time to build a full treatment package. In a drop-out method, clinicians start with the full package and remove components. The best method depends on the learner, the behavior, and the treatment goal.
These methods determine the underlying logic of the experiment, or whether clinicians add or remove components. Then, nested within a broader method, the research design determines how and when clinicians make those changes.
The drop-out method for ABA component analysis
A drop-out analysis tests which components are necessary for behavior change. The clinician starts with the full treatment package and removes components one at a time while measuring behavior. This approach can produce immediate improvement, but may not be appropriate if removing a component could harm the learner.
If you have a treatment package “BC,” the drop-out method begins with the full package, then “drops,” a component. For example: Baseline -> BC -> B. The clinician then applies this logic within a broader research design that determines how and when to add each component.
- Produces immediate improvement:
Because it begins with the full intervention package, the drop-out method can immediately improve behavior.
“In clinical settings, we often want the learner to improve as quickly as possible,” says Haas. “Starting with the full intervention helps you achieve that right away, instead of waiting to build the treatment piece by piece.” - Practical in clinical settings:
Because the learner receives a fully effective intervention at the outset, there is less concern about withholding treatment. This gives the method more social validity, making it more acceptable to caregivers, teachers, and other stakeholders. - Efficient for identifying necessary components:
The drop-out method quickly shows which components you need to maintain treatment progress. - Allows you to simplify complex, resource-heavy interventions:
By removing unnecessary components, clinicians can make interventions easier to implement and maintain. This process helps clinicians apply the principle of parsimony by selecting the simplest intervention that produces effective change.
“Drop-out is very effective when you have an intervention that already works but you want to streamline it,” explains Haas. “In the end, it can help you save time and resources by eliminating parts of your plan that you don’t need. In real-world settings, that means the intervention is more practical for the people implementing it every day.”
Cons of the drop-out method:
- Does not isolate components independently:
Because clinicians evaluate components within the context of the full or partial package, they cannot determine whether a single component would be effective on its own.
“With a drop-out analysis, you’re always evaluating components after the learner experienced them in combination with another,” says Morin. “That means you don’t get a clean test of whether one component alone would produce the same effect, or whether it only appears effective because of its prior pairing with other components in the intervention.” - Asks clinician to remove potentially useful behavior:
To run a drop-out analysis, clinicians must remove components that may be contributing to progress. This can be difficult in practice, especially when the learner is benefiting from the full intervention.
Haas notes that in some cases, dropping a component can even be unethical. “If we’re using an intervention to reduce self-injurious or aggressive behavior, it may not be appropriate to remove a component if that could cause the behavior to increase, even if it would make the intervention more efficient in the long run.”
When to use the drop-out method:
- When you want to simplify an intervention that is already effective
- When your goal is to identify necessary components
- When behavior is not dangerous or high-risk if it temporarily worsens
- When you can ethically remove components without harming the learner
The add-in method for ABA component analysis
The add-in method tests whether a component is sufficient to produce behavior change. The practitioner adds components one at a time to build a treatment package. If behavior improves after adding a component, it may be sufficient. This method is useful for improving interventions but is sensitive to sequence effects.
If you have a treatment package “BC,” the add-in method introduces one component at a time to build toward the full intervention. For example, B → BC. The clinician then applies this logic within a broader research design that determines how and when to add each component.
Pros of the add-in method
- Identifies sufficient components:
The add-in method helps determine whether a component is sufficient to produce behavior change on its own. - Builds the intervention step-by-step:
You can gradually strengthen it until it meets your performance goals. - Avoids withdrawing effective treatment:
Because you are adding components rather than removing them, there is less concern about disrupting progress. - Works with non-reversible behaviors:
This method can be used when behavior is unlikely to return to baseline (e.g., skill acquisition).
Cons of the add-in method
- Slower to produce improvement:
Because you begin with little or no intervention, behavior may not improve right away. - Sequence effects may influence results:
The order in which you introduce components can change how they appear to work,” says Morin. “If you introduce B and then C, the effect of C depends on that sequence, not just on what it does independently. That means that, if behavior is already improving, it also becomes harder to detect the value of new components on their own.”
When to use the add-in method
- When your current intervention is not producing enough improvement
- When you want to build an intervention step-by-step
- When you want to identify which components are sufficient
- When behavior is not reversible
- When you want to avoid removing an effective intervention
Decision matrix on add-in vs. drop-out method
Choosing between add-in and drop-out methods depends on your goal, the learner’s needs, and practical constraints. Add-in builds interventions step by step, while drop-out simplifies existing ones. Use this matrix to decide which method fits your situation, based on behavior type, urgency, and ethical considerations.
Decision matrix on add-in vs. drop-out method for ABA component analysis
How to conduct ABA component analysis, step-by-step
To run a component analysis in ABA, clinicians add or remove parts of an intervention to see which ones change behavior. Most analyses follow the same basic steps: define the treatment, choose a method, collect baseline data, and measure behavior over time.
Here’s a breakdown of the process:
- Define your goal: Start by identifying what you want to learn. For example, are you trying to simplify an effective intervention or determine why an intervention isn’t working? Your goal will guide your method and design.
- Define the treatment package: List all components of the intervention clearly. Each component should be specific and measurable so it can be evaluated on its own. For example, you might define baseline (A) and intervention components (e.g., B, C, D).
- Establish a baseline: Measure the target behavior in its natural state before introducing or modifying the intervention. A stable baseline helps you compare later changes and determine whether a component is effective.
- Select your analysis method: Choose between an add-in or drop-out approach. As a general rule, use a drop-out method to simplify an effective intervention and an add-in method to build or improve one that isn’t working.
For add-in, introduce components one at a time to see which ones are sufficient to cause change. (e.g., B -> BC)
For drop-out, start with the full intervention and remove components to see which ones are necessary. (e.g., BC -> B) - Apply a research design: Your method determines whether you add or remove components. Your design determines how you sequence those changes to maintain experimental control.
The three major research designs include:- Reversal (withdrawal design): Introduce or remove conditions across phases, and then reverse the process (e.g., BC -> B -> BC).
- Alternating (multielement design): Alternate conditions rapidly across sessions.
- Multiple baseline: Introduce the component at different times across different baselines (e.g., different behaviors, settings, or participants).
We describe each design in detail below.
- Systematically manipulate variables: Introduce or remove components according to your method and design.
- Evaluate the change: Compare behavior across conditions to determine whether a component produces meaningful change. Focus on level, trend, and consistency.
- A component is active if adding or removing it changes the behavior you’re measuring.
- A component is necessary if removing it causes behavior to return toward baseline.
- A component is sufficient if adding it alone yields an improvement.
How to implement different research designs in ABA component analysis
In an ABA component analysis, the research design shows how clinicians test changes in components. A reversal design adds and removes conditions, an alternating design compares them across sessions, and a multiple baseline design staggers changes. Clinicians use these designs within an add-in or drop-out method.
Component analysis typically uses a single-subject research design (SSRD) to evaluate behavior change within an individual learner. In SSRDs, researchers vary the intervention over time rather than comparing groups. Some designs, such as multiple baseline, can include several participants, but still analyze each one individually.
Steps to implement reversal design in ABA component analysis
A reversal design tests components by adding them, removing them, and then adding them back across phases. Clinicians collect baseline data, change one component at a time, and keep each condition in place for several sessions. This design provides strong evidence and helps isolate the effect of a component over time.
“Reversal designs are one of the strongest ways to isolate the effect of a component because you repeatedly introduce and remove it and observe how behavior changes,” says Morin.
While it is a highly robust design, Morin cautions that clinicians must account for potential confounding factors:
“In reversal designs involving more than two components – also called a ‘multitreatment’ design – you can’t directly compare non-adjacent phases, such as Phase 3 and Phase 1. The behavior also has to be reversible — meaning it will return to baseline when the intervention is removed. That’s why this design doesn’t work well for things like skill acquisition, where the learner won’t ‘unlearn’ the skill.”
Here’s a step-by-step overview of the reversal design, for both the drop-out and add-in methods:
- Define the intervention components
Identify all components in the treatment package (e.g., B and C). - Collect baseline data
Measure behavior without intervention to establish a comparison point. - Determine when to change phases
Decide in advance how you will know when to move to the next phase. Set clear criteria, such as a stable pattern across sessions or meeting a target performance level. Wait until behavior shows a steady pattern before adding or removing a component. - Implement the first condition
- Drop-out: start with the full package (BC)
- Add-in: start with baseline or a single component (B)
Collect data across multiple sessions.
- Change the condition
- Drop-out: remove a component (BC → B)
- Add-in: add a component (B → BC)
Continue collecting behavior data across multiple sessions.
- Reverse the condition
- Drop-out: reintroduce the component (B → BC)
- Add-in: remove and re-add if needed (BC → B)
Observe whether behavior changes again. At this point, you have completed a full reversal sequence. For example, with three sessions per component: - Drop-out: BC, BC, BC -> B, B, B -> BC, BC, BC
- Add-in: B, B, B -> BC, BC, BC -> B, B, B
- Interpret the results:
Track and graph behavior for each condition separately. Look for clear differences in the behavior across conditions. If behavior changes consistently with each condition change, this supports a functional relation and shows whether a component is necessary (drop-out) or sufficient (add-in).
Steps to implement alternating (multi-element) design in ABA component analysis
An alternating (multi-element) design tests components by switching between them across sessions. Clinicians collect baseline data, alternate one component at a time, and compare performance across sessions. This design allows for faster comparisons and helps identify which components produce change without keeping each condition in place for multiple sessions.
Some authors and researchers treat alternating (multi-element) designs as a form of comparative analysis, used to compare two or more distinct interventions. Others apply the component analysis label when alternating conditions are used to evaluate parts of a treatment package, often within a larger withdrawal or multiple baseline design. Given the source differences, we are including alternating designs in our discussion to give the full picture.
Haas says that the multi-element design is often useful in clinical settings. “You can use a multi-element design when you have several interventions you think might work,” she explains. “If more than one works, it also gives you flexibility—you can involve the learner in choosing which one to continue, which can make the intervention more acceptable and easier to implement.”
Here’s a step-by-step overview of the alternating design for both the add-in and drop-out methods:
- Define the intervention components
Identify all components in the treatment package (e.g., B and C). - Collect baseline data
Measure behavior without intervention to establish a comparison point. - Implement the first condition
- Drop-out: start with the full package (BC)
- Add-in: start with baseline or a single component (B)
- Alternate conditions
Rotate conditions rapidly across sessions (e.g., BC, B, BC, B). Keep sessions short and consistent so you can compare results. Collect data during each session.- Drop-out: remove a component (BC → B)
- Add-in: add a component (B → BC)
- Compare performance
Track and graph behavior for each condition separately. Look for clear differences in level and trend across conditions. - Identify active components
Determine which components produce the strongest and most consistent effects. Components that lead to better performance across sessions are likely active.
Steps to implement multiple baseline design in ABA component analysis
A multiple baseline design tests components across different learners, behaviors, or settings. Clinicians introduce the same component at different times for each baseline, rather than all at once. One baseline starts first while others stay unchanged. This timing helps show that the component causes behavior change without removing the intervention.
Dr. Haas highlights a key tradeoff in multiple baseline designs in clinical settings: they allow clinicians to maintain effective interventions for some learners, but may delay support for others. “Once an intervention starts working for one learner, you don’t have to take it away, you can keep it in place and still demonstrate control by introducing it later with others. But because you’re staggering the intervention, other learners remain in baseline, and if the behavior needs to be addressed quickly, that delay isn’t always appropriate.”
Here’s a step-by-step overview of the multiple baseline method, for both the drop-out and add-in methods:
- Define the intervention components
Identify all components in the treatment package (e.g., B and C). - Select your baselines
Choose the behaviors, settings, or learners you will include in the analysis. In this example, we will use multiple participants. - Implement the first condition
- Add-in: Introduce the component (B) only in the first baseline (first participant).
- Keep all participants in the baseline stage.
Collect data across multiple sessions.
- Stagger the intervention
Introduce the component in the remaining baselines one at a time, only after stable responding in each prior phase.
Example:- Learner 1: Baseline -> B
- Learner 2: Baseline -> Baseline -> B
- Learner 3: Baseline -> Baseline -> Baseline -> B
- Compare performance
Evaluate whether behavior changes only after you introduce the component. - Repeat as needed
Add additional components or extend the design to test other parts of the intervention. - Identify active components
Determine whether behavior changes only after you introduce the component in each baseline. If the same improvement occurs across learners, behaviors, or settings, this suggests the component is responsible for the change.
ABA component analysis readiness checklist
Our ABA component analysis checklist condenses what you need to know about getting started with component analysis into a single-page document. Use it to choose the right design for your goals and ensure you meet the basic requirements for experimental control.
Download our ABA component analysis readiness checklist to make sure your design is sound and you’re ready to move forward with confidence.
[fs-toc-omit]Examples of ABA component analysis
Component analysis helps clinicians and researchers break down complex interventions and identify what actually drives behavior change or skill acquisition. These examples show how practitioners apply both add-in and drop-out methods to refine treatment, reduce unnecessary steps, and improve outcomes for real-world learners.
Here are three examples of clinicians and researchers using ABA component analysis to inform their treatments:
- Teaching conversational skills
This example comes from a 2013 study, “A component analysis of a behavioral skills training package used to teach conversation skills to young adults with autism spectrum and other developmental disorders,” published in the Journal Research in Autism Spectrum Disorders.
Goal: To improve conversation skills in young adults with autism and identify which components of a training package were necessary.
Method: Researchers created a behavioral skills training (BST) package with four components: instruction, modeling, rehearsal, and feedback. They used a multiple baseline design across participants with an add-in component analysis, introducing components one at a time (e.g., instruction → instruction + modeling → full package) and measuring behavior change at each step. They progressed each participant through the sequence after observing stable responses and staggered the timing across participants to establish experimental control without requiring reversal.
Outcome: Their analysis showed that different participants required different combinations of components to reach criterion performance, and no single component consistently produced behavior change across all participants.
Result: This analysis suggested that the most effective components varied by individual, and that implementing the full training package may be more efficient than isolating individual components in practice. - Increasing food acceptance in children
This example comes from a 1995 research article, “Use of component analyses to identify active variables in treatment packages for children with feeding disorders,” published in the Journal of Applied Behavior Analysis.
Goal: To increase food acceptance and consumption in children with developmental disabilities and identify which components of a feeding intervention are necessary.
Method: Researchers implemented a drop-out component analysis by first introducing a full treatment package that included multiple components (e.g., choice, attention, escape extinction, and warm-up procedures). They then systematically removed individual components and compared performance across conditions (e.g., full package vs. package without one component).
Outcome: They found that removing most components had little effect on food acceptance, but removing escape extinction led to a clear decrease in performance.
Result: This analysis showed that escape extinction was the critical (necessary) component, allowing clinicians to simplify the intervention by removing less effective elements while still providing effective treatment. - Behavioral skills training for clinical procedures
This example comes from a 2012 research article, “Component analysis of behavior skills training in functional analysis,” published in Behavioral Interventions.
Goal: To determine which components of a behavioral skills training (BST) package are necessary to teach teachers to conduct functional analyses correctly.
Method: Researchers created a BST package that included instruction, modeling, rehearsal, and feedback. They used an add-in component analysis, introducing components step-by-step (e.g., instruction → instruction + modeling → full package). Within this sequence, they embedded an alternating-treatments design, meaning they rapidly alternated between components to compare their effects. This allowed them to evaluate both the combined and independent effects of each component without relying on the longer reversal design.
Outcome: Their analysis showed that feedback was a necessary component, while instruction and modeling alone were not sufficient.
Result: This analysis helped identify the most effective components of the training package. With this information, researchers and instructors can focus instruction on practice and feedback without reducing the overall program's efficacy.
[fs-toc-omit]When to use other ABA analysis types
Component analysis helps you identify which parts of a treatment package matter, but it is not always the best choice. In some cases, you may want to adjust the intensity of a single intervention or compare entirely different interventions. In those situations, parametric or comparative analyses may be more appropriate.
Component analysis vs. parametric analysis
A component analysis examines which parts of a multi-component intervention drive behavior change. In contrast, a parametric analysis evaluates how different levels or intensities of a single intervention affect behavior. Use a parametric analysis when you want to adjust how you deliver an intervention.
Use component analysis to determine which elements of a treatment package are necessary or effective. For example, you might test whether prompting, reinforcement, or both are responsible for behavior change.
Use a parametric analysis when you already know which intervention to use but want to refine it. For example, you might adjust the schedule or magnitude of reinforcement to see how those changes influence behavior.
Component analysis vs. comparative analysis
A component analysis examines how individual parts of a single treatment package affect behavior. A comparative analysis evaluates two or more separate interventions to determine which one produces better outcomes.
“A lot of people mix up components and comparative analysis,” says Morin. “Comparative analysis is about choosing between entirely different interventions, while component analysis is about figuring out what component is actually doing the work within one treatment.”
[fs-toc-omit]Visualizing ABA component analysis results
To visualize ABA component analysis results, collect data during baseline and each subsequent phase. Clinicians often record frequency and convert it to a percentage. Plot the data across sessions and add phase change lines to mark condition shifts, then visually inspect how behavior changes as components are added or removed.
Here’s an overview of how to gather data and graph the results:
- Graph and prepare your data
Start by selecting a clear dependent variable, such as percent correct, rate, or frequency. Record data consistently across sessions within each phase. If needed, convert raw counts into percentages to keep results comparable. For example, you can convert frequency data into the percentage of the session during which the behavior occurred. - Plot the data
Use a simple line graph with sessions on the x-axis and the target behavior on the y-axis. Plot one data path that connects points within each phase. Do not connect lines across phase changes. Each phase should stand on its own. - Add phase change lines
Insert vertical phase lines between sessions where conditions change. These lines separate phases (e.g., BC → B → BC) and show exactly when you introduce or remove a component. Place them between sessions, not on data points. - Visually analyze the results
Examine changes in level, trend, and variability across phases. Look for immediate and consistent shifts in behavior following a phase change. These patterns help determine whether adding or removing a component influenced behavior.
Examples of ABA component analysis graphs
Drop-out and add-in reversal designs show different patterns on a graph. In a reversal design, behavior changes as a component is removed and then added back. In an add-in design, behavior changes step by step as new components are introduced. The examples below show how these patterns appear across phases and sessions.
Example of a drop-out ABA component analysis graph with reversal design
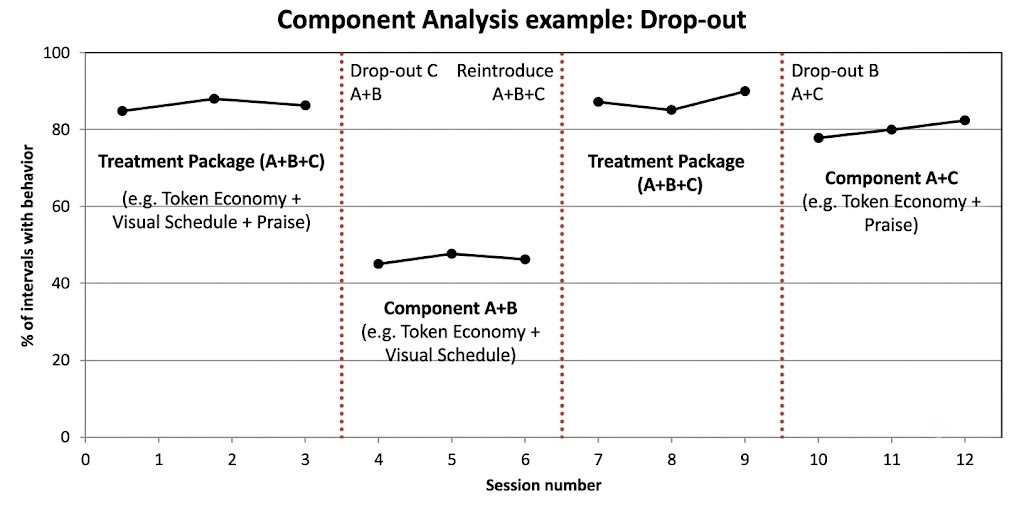
The graph shows the percentage of intervals in which a student follows the teacher’s instructions during class. During baseline, the student follows instructions at low levels. When a clinician introduces the full intervention package (component B - reinforcement and component C - prompting), the student follows instructions more often. When the teacher removes prompting, they follow instructions less often, only to increase after the teacher reintroduces prompting. This suggests that prompting is a necessary component.
Example of an add-in ABA component analysis graph with reversal design
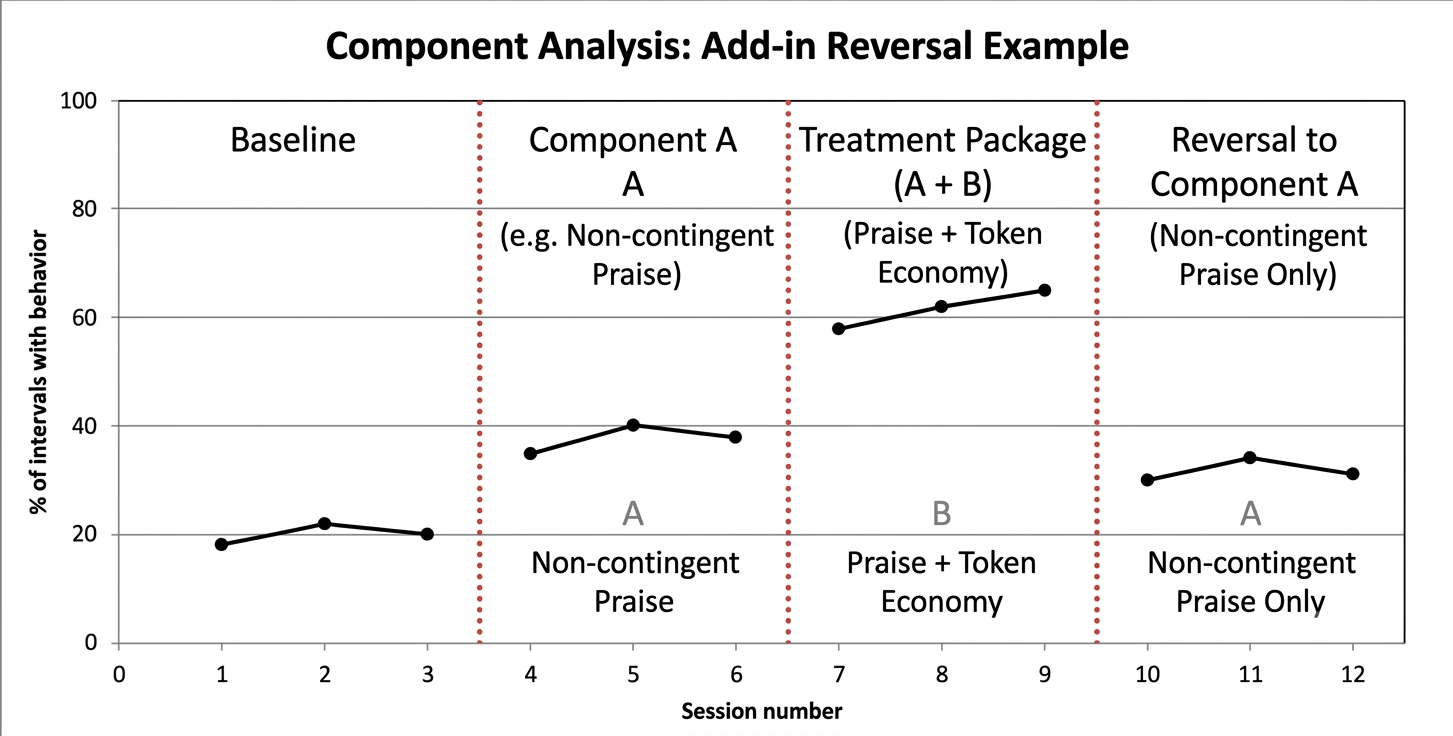
The graph shows the percentage of intervals in which a student completes assigned tasks independently. During baseline, performance remains low. When the teacher introduces prompting (B), performance increases. When the teacher adds reinforcement (BC), performance improves further. When the teacher removes reinforcement and returns to prompting alone, performance decreases, showing that reinforcement strengthens the effect of prompting.
ABA component analysis graph template
Our free ABA component analysis graph template provides a clear structure for plotting your component analysis data across sessions. It includes built-in spaces for phase change lines and supports both add-in and drop-out (reversal) designs. Use it to organize data, label conditions, and visually evaluate how components affect behavior.
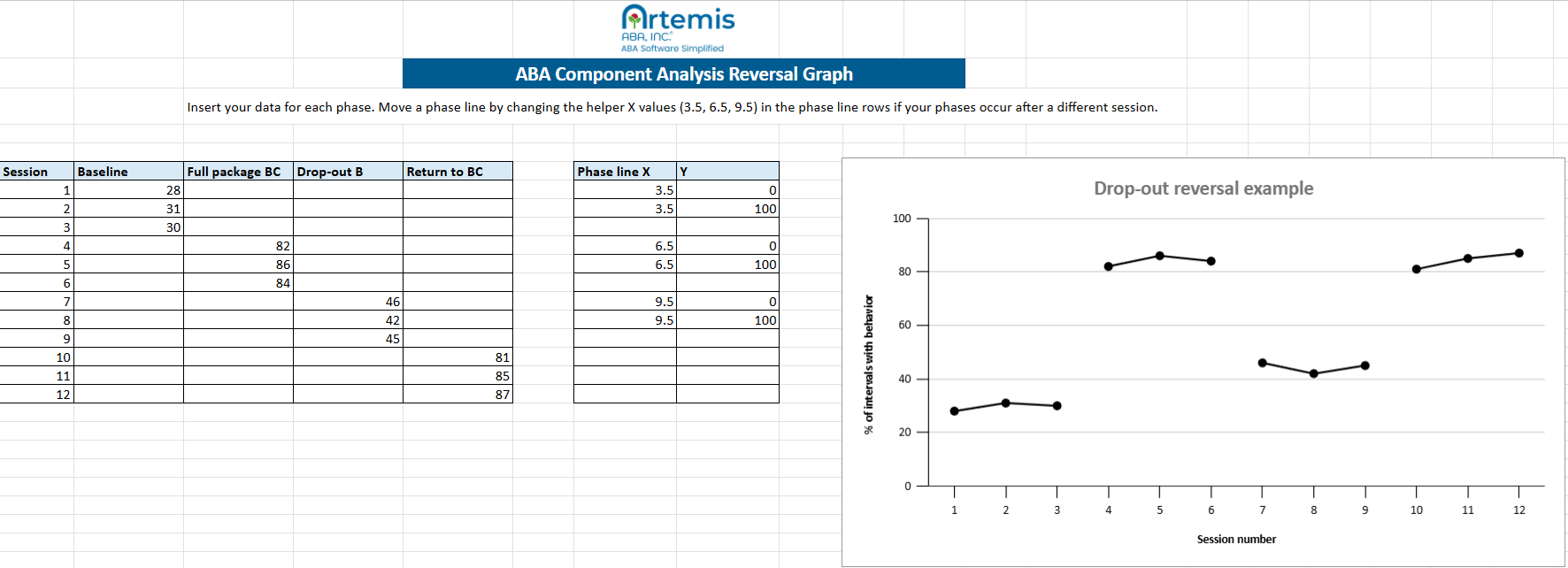
Download our free ABA component analysis graphing template to start visualizing your data and evaluating how each treatment component affects behavior.
How to streamline ABA component analysis with Artemis ABA
When you’re ready to move beyond manual spreadsheets, Artemis ABA gives clinicians the tools to run cleaner, more precise component analyses. As clinicians move between phases, Artemis ABA’s platform organizes your data by condition so you can clearly see how each component affects behavior.
With built-in graphing, real-time updates, and side-by-side phase comparisons, you can quickly detect meaningful changes and determine whether adding or removing a component improves outcomes. This makes it easier to isolate what’s working and avoid overcomplicating treatment.
Artemis ABA turns complex phase data into clear visual patterns, helping you make faster, more confident decisions about how to adjust and refine interventions for each learner.
Schedule Your Walkthrough

FAQ on ABA component analysis
How many data points are required before changing a phase in ABA component analysis?

It depends on your goal. If you are conducting a research-focused analysis and need strong experimental control, you should collect at least three data points per phase, and more if needed to show a stable pattern. In clinical settings, where the goal is to improve outcomes, clinicians may switch phases sooner based on the learner’s progress and practical needs.
When is it ethically inappropriate to use a drop-out component analysis?
It is ethically inappropriate to use a drop-out component analysis when removing a component could put the learner at risk, such as in cases involving self-injurious or aggressive behavior. Because this method requires withdrawing part of an effective intervention, it may lead to a return of harmful behavior, which raises serious safety concerns.
How do you identify sequence effects in your component analysis data?
You identify sequence effects by looking for patterns where the order of conditions influences behavior rather than the components themselves. For example, if a component appears more effective only when it follows another condition, that may indicate a sequence effect. You can address this by using a counterbalanced design, in which you repeat the analysis but introduce components in the opposite order to your first design. This process helps you see whether the effects remain consistent, regardless of the sequence.
Monday to Friday, 7 AM – 7 PM CST.
If you're reaching out outside these hours, please submit a support ticket—our team will respond as soon as possible.


%201.webp)


