


Using ABA Functional Analysis: How-to, Examples, and Streamlining
Inside this article:

Learn how to set up and run a functional analysis (FA) in ABA. Explore how to use FA in your practice and when to choose other methods, and read expert best practices on how to run and interpret an FA. See how to interpret graphs to guide treatment.
Executive summary:
A functional analysis (FA) is a structured, experimental method used to identify why a behavior occurs by testing how different consequences affect it. Clinicians change one condition at a time and observe when behavior increases to determine its function. While an FA is one of the most accurate ways to assess behavior, it requires time, training, and controlled conditions. In practice, clinicians often use interviews and observation first, then turn to an FA for complex or unclear cases. The results guide behavioral intervention plans and support effective treatment.
[fs-toc-omit]Purpose of functional analysis in ABA
A functional analysis (FA) in ABA uses a step-by-step, experimental approach to determine why a behavior occurs. Clinicians set up situations to evoke the behavior and observe what triggers and maintains it. They use this information to teach more appropriate behaviors that meet the same need and guide effective treatment.
Brian Iwata developed the functional analysis (FA) methodology in the mid-1980s to determine the purpose of self-injurious behavior (SIB). Functional analysis is based on the principles of operant conditioning, where consequences influence whether a behavior increases or decreases. Today, it remains one of the most controlled and evidence-based methods for determining the function of behaviors, including problem behaviors associated with autism spectrum disorders (ASD).
Clinicians use the result of an FA to inform behavioral intervention plans (BIP). Usually, clinicians implement differential reinforcement strategies to strengthen more appropriate behaviors while reducing problem behavior, such as using functional communication training (FCT) to teach a learner how to make requests appropriately, while also using extinction to withhold reinforcement for the problem behavior. Among methods for determining function in ABA, functional analysis is the most accurate but also requires the most time, effort, and resources. Because of these challenges, ABA practitioners usually don’t conduct full functional analyses in typical clinical settings, but rely on FA variations and other methods.
ABA functional analysis (FA) vs. functional behavior assessment (FBA)
A functional behavior assessment (FBA) refers to the broad process of identifying a behavior’s function through methods such as interviewing and observation. A functional analysis (FA) is a specific method that technically falls within an FBA. Clinicians use an FA when other methods do not clearly identify the behavior’s function.
A functional behavior assessment (FBA) is an umbrella term for any method that ABA practitioners use to assess a behavior's function. However, in practice, clinicians often treat and discuss FAs and FBAs as separate methods because an FA requires more time, structure, and resources than other, more typical FBA methods.
When to use FBA indirect and direct assessments
When clinicians start an FBA, they aim to accurately identify a behavior’s function using the least amount of time and resources. In practice, they rely on indirect assessments, such as caregiver interviews and questionnaires, and direct assessments, such as observing the behavior in everyday settings.

Dr. April Haas, BCBA-D, LBA-TX, strongly recommends that clinicians pair direct and indirect assessments in an FBA to strengthen their conclusions.
“Indirect tools like the Questions About Behavioral Function (QABF) questionnaire give us a starting point, but any interview can be biased, and it rarely confirms the function on its own,” Haas says. “Direct observation lets us test those ideas by watching the behavior as it plays out naturally.”

Jelisia Thompson, BCBA, LBA, says that clinicians run direct assessments – or observe behavior in a natural environment – to collect antecedent-behavior-consequence (ABC) data.
“During a direct assessment, we examine what occurs immediately before the behavior, what the behavior looks like, and what happens right after. After collecting ABC data, I often use tools like bar graphs as a visual representation to compare interfering behaviors, assist in determining the function, and guide the development of an intervention strategy.”
Haas says the length of an FBA depends on the behavior’s pattern. “I can sometimes gather enough data in one day for a behavior a learner performs very frequently. In other cases, it might take me closer to a week because I want to observe the learner across different settings.”
When to use functional analysis (FA)
Unlike other methods in an FBA, in which the clinician does not intentionally evoke a behavior, a traditional functional analysis follows an experimental design in which clinicians deliberately evoke the problem behavior. It is the gold standard for rigorously assessing a behavior's function, but it is resource- and time-intensive and potentially stressful for the learner.
In practice, clinicians use an FA only when interviews and direct observation do not clearly identify the function. However, it may be necessary for complex or severe behaviors when the function is unclear. Even when clinicians do not run a full FA, they often adapt parts of it to fit real-world settings and make the process more practical.
Setting up a functional analysis in an ABA setting
To set up a functional analysis, a clinician creates a controlled environment to isolate and test specific functions without distractions. Ideally, they run trials in a quiet, empty room. In practice, clinicians adjust this design to accommodate the practical limitations of common ABA environments, such as clinics and schools.
A functional analysis follows an experimental design in which clinicians systematically compare test conditions to a neutral control. By isolating variables and observing behavior across conditions, they identify cause-and-effect relationships.
For example, clinicians compare the control condition to test conditions that assess possible functions of behavior, such as attention, access to items, sensory input, and escape. In each condition, the clinician delivers a consequence that matches a possible function. This may include positive reinforcement, such as giving attention or access to an item, or negative reinforcement, such as removing a task or demand. If the behavior increases after a specific consequence, that consequence likely reinforces the behavior and points to its function.
To keep other variables consistent, clinicians conduct a functional analysis in a highly controlled environment. In practice, however, several constraints make it difficult to maintain this level of experimental control.
“Technically, you are supposed to run an FA in a ‘control room,’ with nothing in it except for a table, a chair, and, ideally, a two-way glass that allows another clinician to observe, but that the learner can’t see through,” explains Haas. “It’s very hard to create these strict environmental conditions in an ABA setting like a clinic.”
Hayden Heath, M.S., BCBA, LBA-TX, notes that other real-world constraints often make it difficult to create a truly controlled, distraction-free environment during a functional analysis. In practice, you don’t always have the ability to create a perfectly controlled environment.

“I’ve had cases where the environment itself becomes a variable you can’t control,” Heath says. “For example, we had a very young child who didn’t want to be separated from their parents. They wouldn’t participate unless their parents were in the room. In those situations, you have to adapt – trying to force a perfectly controlled setup isn’t always practical or clinically appropriate.”
The standard conditions of an ABA functional analysis
An ABA functional analysis includes four test conditions: attention, escape, tangible, and sensory (alone), plus a control (“play”) condition. In each test condition, the clinician changes one variable, such as giving attention or removing a task. By tracking when the behavior occurs most often, the clinician identifies which consequence reinforces it.
Here are the details of the standard conditions of an ABA functional analysis:
Exploring the standard conditions in an ABA functional analysis
Alternative formats of functional analysis in ABA
Researchers and clinicians have adapted the traditional functional analysis to address limitations such as time constraints, risk, and lack of environmental control. These variations include multi-element, trial-based, brief, latency, and IISCA analyses. Clinicians choose the format that best fits their setting, available time, and the behavior they are assessing.
Different functional analysis methods vary in key ways, including their experimental design, setting, and stopping criteria. These differences often involve how the clinician arranges sessions and conditions.
For example, many methods use a multi-element design, in which the clinician alternates between conditions across separate sessions, whereas others use a pairwise design, in which the clinician directly compares two conditions within the same session or trial. Some methods require a controlled, distraction-free setting, while others can take place in natural environments such as homes or classrooms. These variations affect whether the assessment is faster, safer, more accurate, or more practical to implement in real-world settings.
In the 2025 paper “Functional Analysis Decision-Making Considerations,” the authors identify several key factors clinicians should consider when selecting an FA method, including accuracy, time availability, the severity of the behavior, the frequency of the behavior, and more. The authors also emphasize that this list is not exhaustive and that additional variables, such as caregiver preference and clinical context, may influence decision-making. Ultimately, they stress that clinicians often choose from a range of modified or alternative FA formats based on the needs of the individual case.
Below is a brief overview of several commonly used FA methods and when clinicians might consider each one. These summaries provide a general introduction; clinicians should review the full procedures and supporting research for each method before implementing them in practice.
Traditional ABA functional analysis format
In a traditional functional analysis, the clinician tests different conditions that may affect behavior using a multi-element design in a controlled, low-distraction room. The clinician runs each condition as a short session, usually lasting 5 to 10 minutes.
After each session, the clinician switches to a different condition instead of repeating the same one right away. The clinician rotates through conditions in a repeated sequence, or cycle (for example: escape, attention, play, tangible, alone). The clinician runs sessions back-to-back in the same space and may perform brief resets between sessions. The learner usually stays in the room while the clinician quickly changes materials or demands.
After completing one full cycle, the clinician repeats the cycle until they’ve tested each condition across multiple sessions, typically 3 to 5 times.
During each session, the clinician or an outside observer collects continuous data on how frequently the learner engages in the behavior. The clinician compares behavior across conditions to determine which situation consistently produces the highest levels of behavior. Higher and stable responding in a specific condition indicates that the outcome associated with that condition likely maintains the behavior.
Advantages:
- Provides strong experimental control and clear demonstration of behavioral function
- Allows direct comparison across multiple conditions
- Considered the most well-established and widely researched FA method
- Produces highly reliable and valid results when implemented correctly
Limitations:
- Requires more time, training, and resources than other FA methods
- May evoke higher rates of challenging behavior
- Can be difficult to implement in natural settings such as classrooms or homes
- May not be appropriate for severe or dangerous behavior
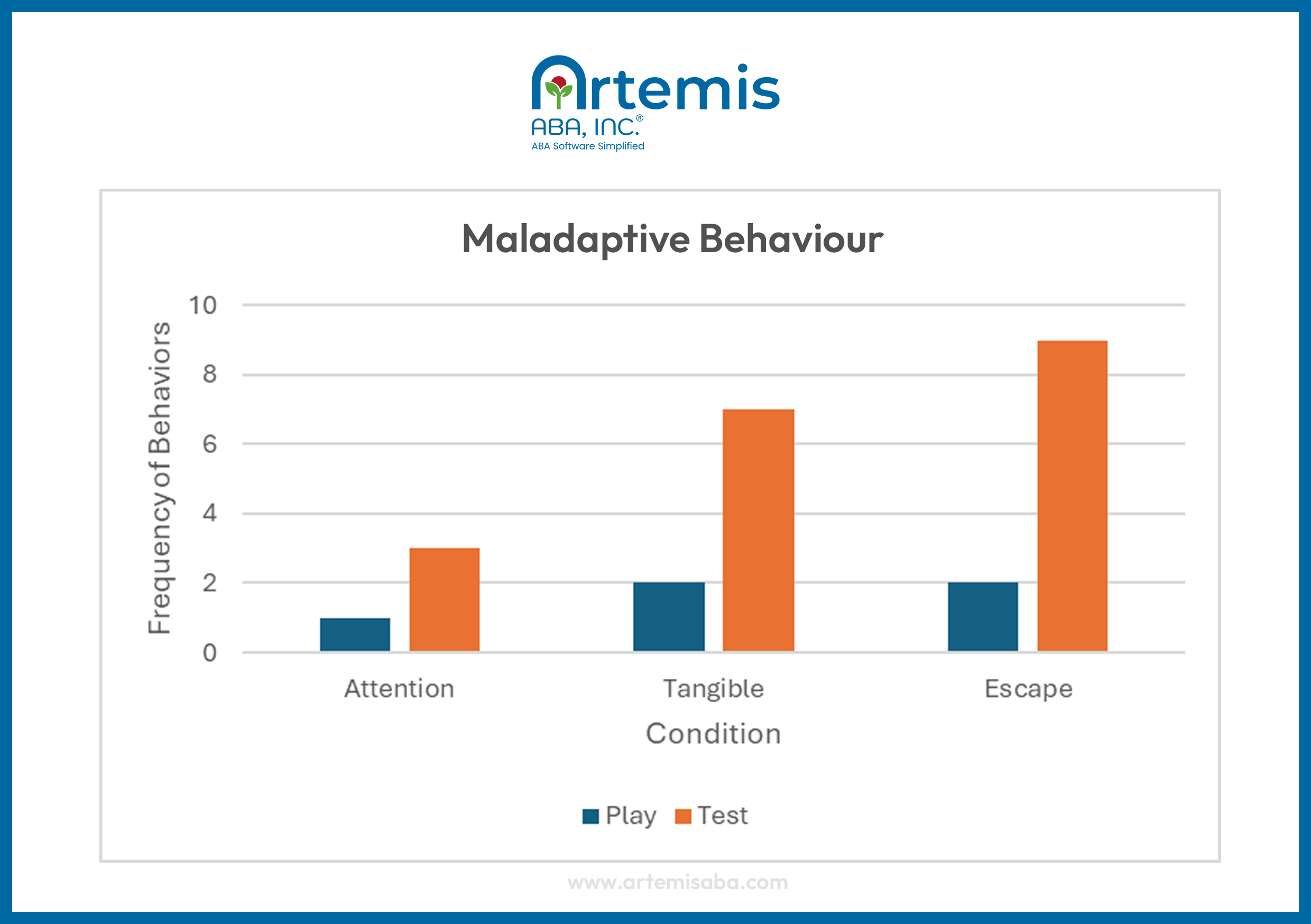
Example of a traditional functional analysis multi-element graph
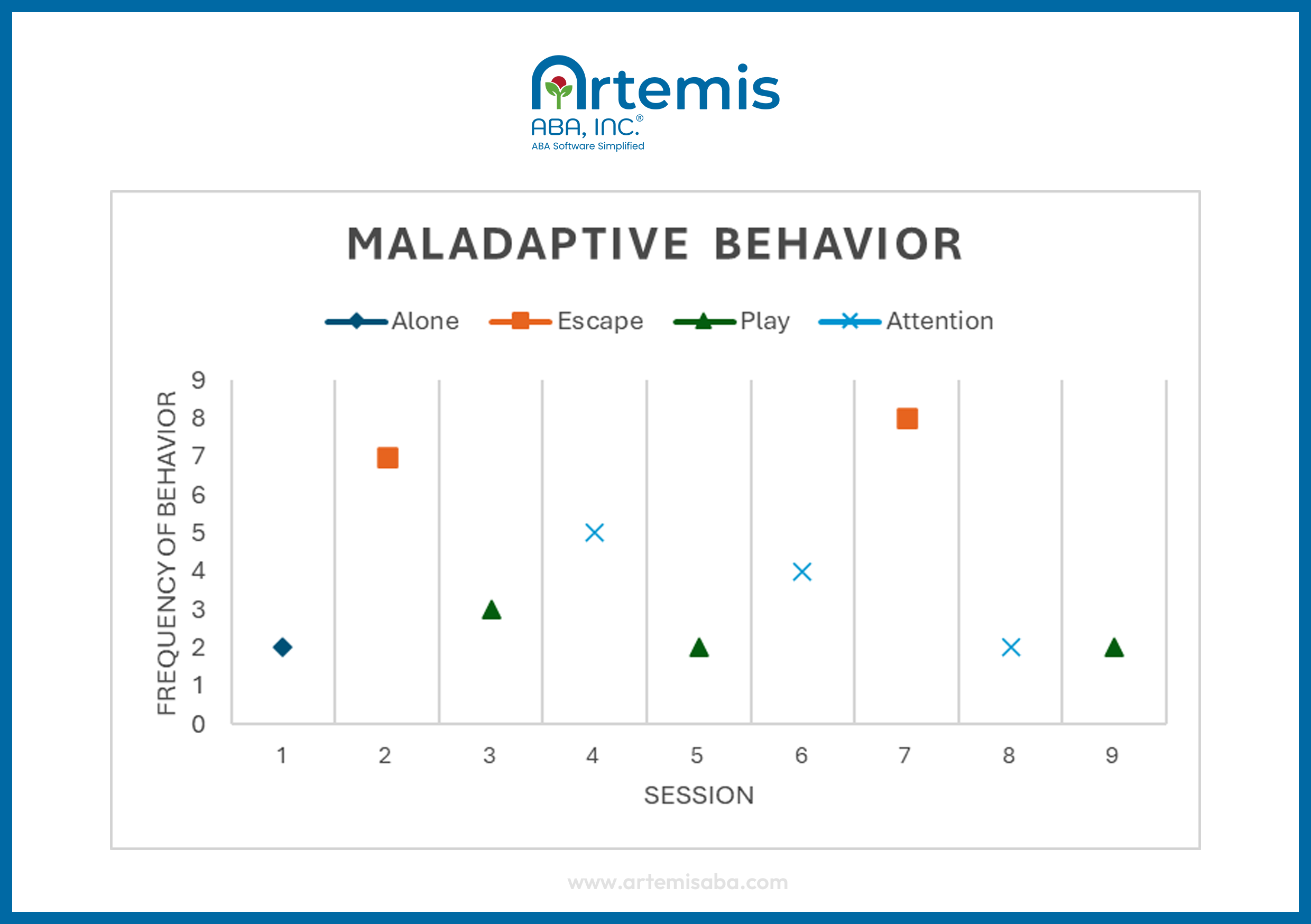
Brief ABA functional assessment (BFA) format
In a brief functional analysis, the clinician also uses a multi-element design, like in a traditional FA, but they run each condition for a short period of time, usually a few minutes, and may only have one or two sessions per condition.
The clinician compares behavior across these conditions to identify likely functions within a limited time frame. Unlike longer functional analyses, the clinician completes the entire assessment in a single session, typically within 60 to 90 minutes.
Advantages:
- Highly time-efficient
- Especially useful for learners who can communicate well
Limitations:
- Doesn’t work well for low-frequency behaviors because of the short observation window
- Short observation window can reduce accuracy
Example of a brief functional analysis (BFA) graph
Trial-based ABA functional assessment format
In a trial-based functional analysis, the clinician runs a series of brief trials using a pairwise format, with each trial consisting of two segments: a control segment followed by a test segment. The clinician embeds these trials into the learner’s daily routine, such as during classroom instruction, rather than conducting them in a separate setting. Each segment lasts a few minutes, allowing the clinician to compare behavior across conditions within the same trial.
Advantages:
- Efficient and time-limited (often around 60 minutes total)
- Requires fewer resources and staff
- Easy to implement in natural settings like homes or schools
Limitations:
- May not capture low-frequency behaviors
- Short trials may not always evoke the behavior
- Results can vary from moderate to high accuracy
Example of a trial-based functional analysis graph
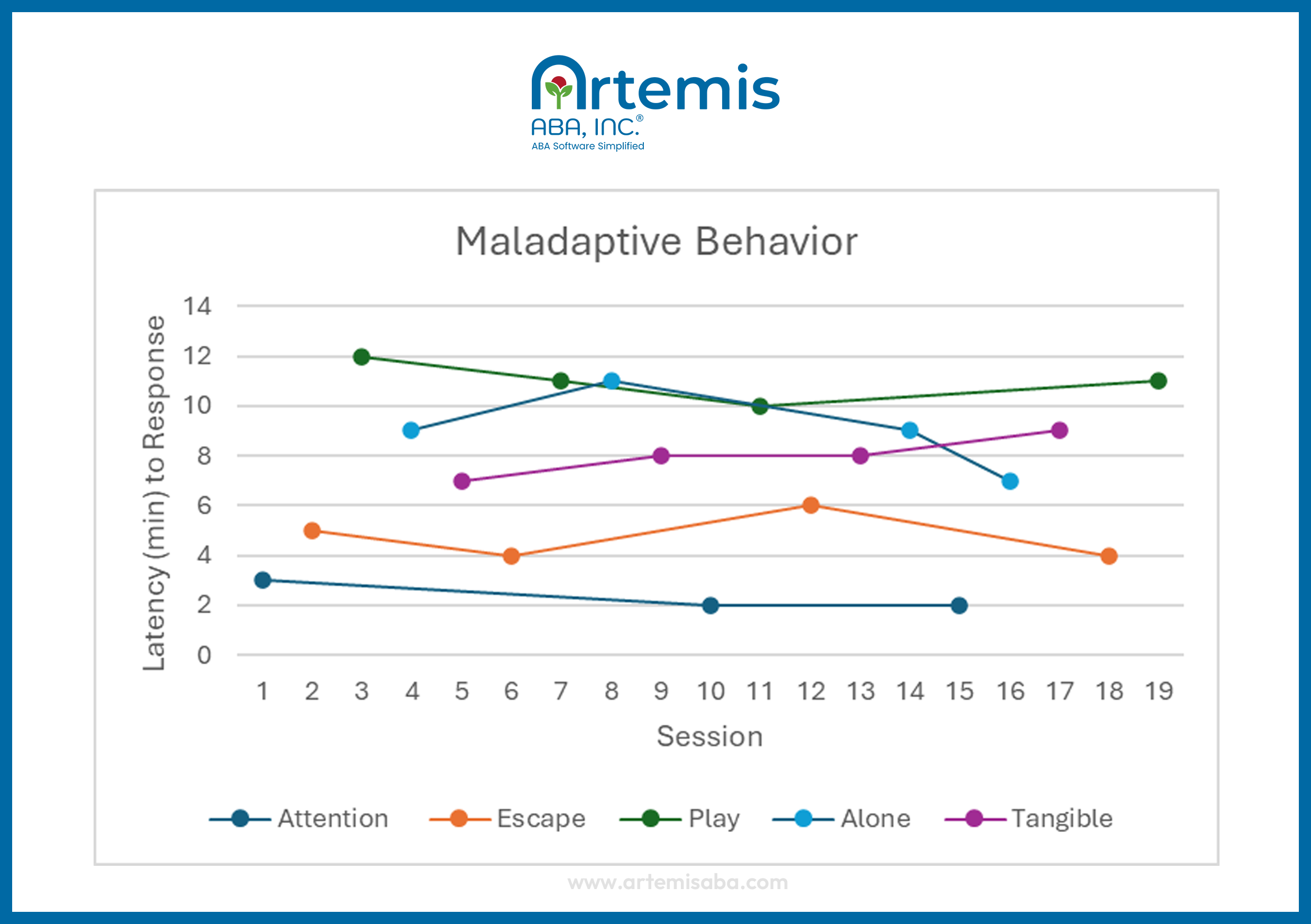
Latency ABA functional assessment format
In a latency-based functional analysis, the clinician measures how long it takes for the learner to show the first instance of challenging behavior after setting up a specific situation.
The clinician begins each session by creating that situation (for example, giving work, withholding attention, or leaving the learner alone) and starts a timer. As soon as the learner engages in the behavior, the clinician stops the timer, ends the session immediately, and provides the outcome associated with that situation (such as a break or attention). The clinician repeats this process across different situations and across multiple sessions to compare how quickly the behavior occurs in each one.
Advantages:
- Reduces the number of times the learner engages in behavior
- Useful for high-risk behavior
- Useful for behaviors that occur at a low rate
- Produces accurate results that often align with traditional functional analyses
Limitation:
- Captures only one response per session, which can make interpreting a causal relationship difficult
Example of a latency functional analysis graph
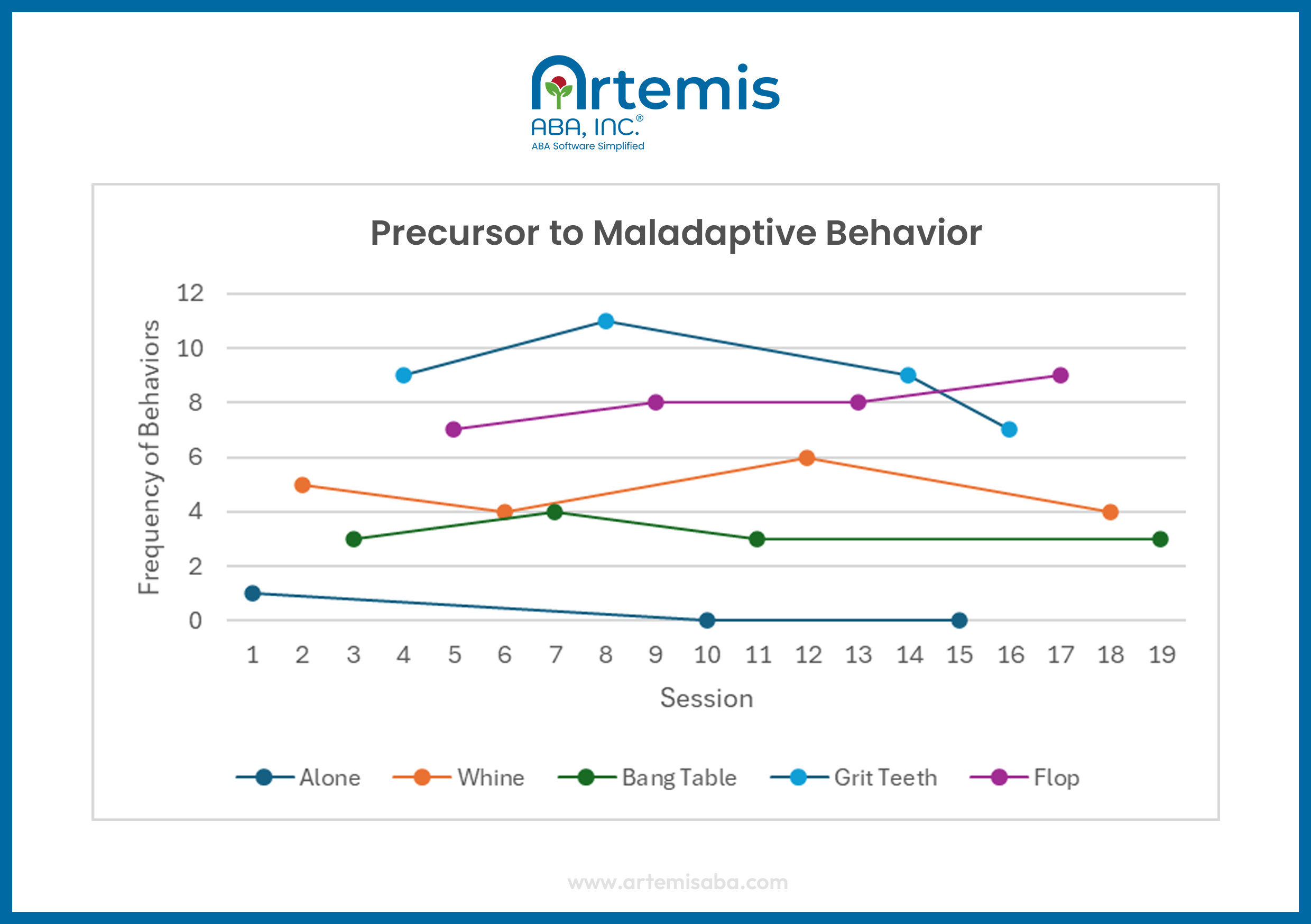
Precursor functional analysis format
In a precursor functional analysis, the clinician identifies and tests early behaviors that happen right before more severe challenging behavior. The clinician selects a precursor that reliably occurs before the more dangerous behavior (for example, picking up an object before throwing it) and uses that behavior during the assessment instead of waiting for the severe behavior to occur.
The clinician begins each session by setting up a specific situation (such as giving work or withholding attention). When the learner engages in the precursor behavior, the clinician immediately provides the outcome associated with that situation (such as a break or attention). The clinician does not wait for the severe behavior to occur.
The clinician repeats this process across different situations and across multiple sessions to determine which outcomes maintain the behavior.
Advantage:
- Useful for high-risk behavior because it does not require the learner to perform the behavior
Limitation:
- Must establish a reliable precursor, which can be difficult and time-consuming
Example of a precursor functional assessment graph
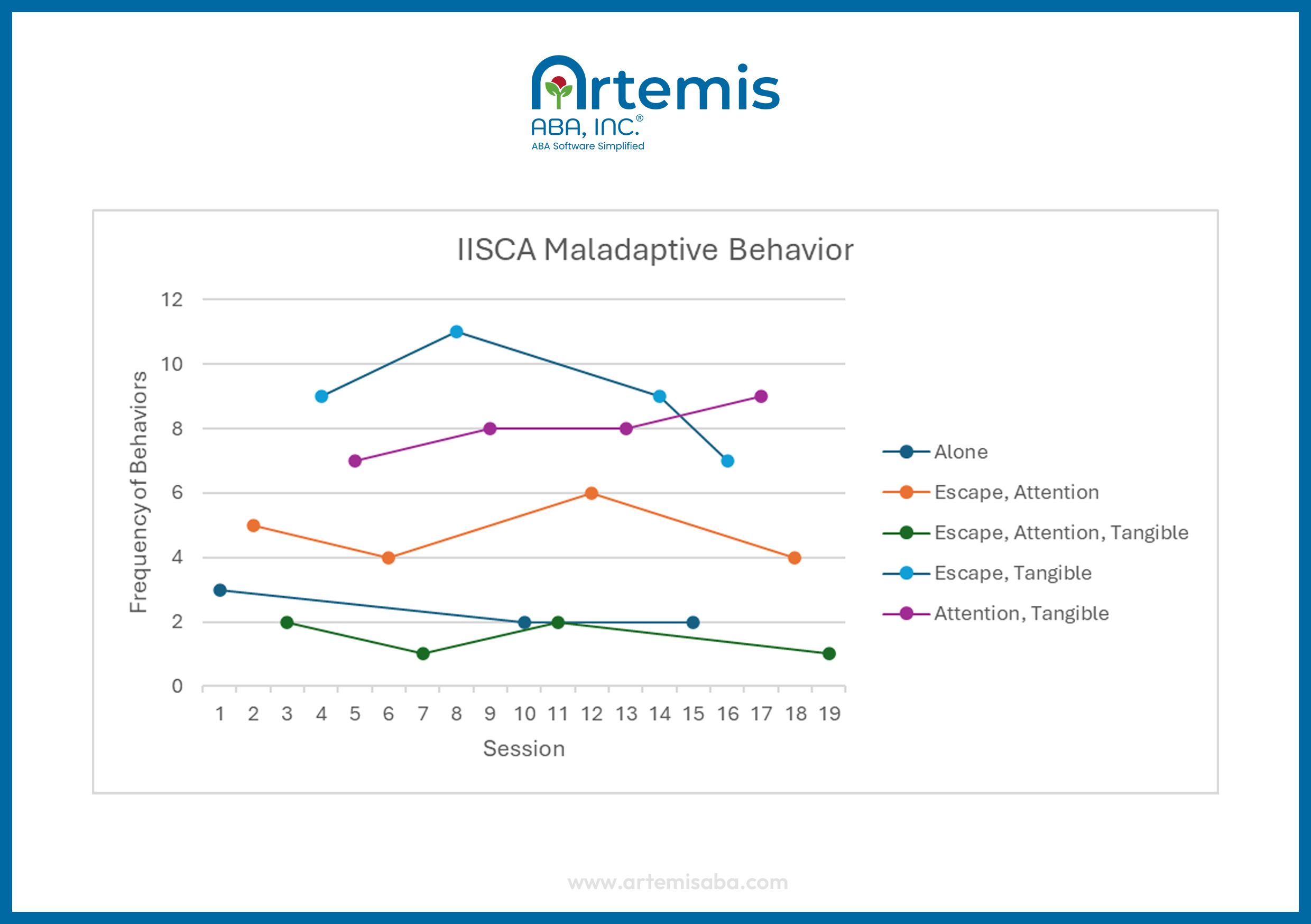
Interview-informed synthesized contingency analysis (IISCA) format for ABA
In a synthesized contingency functional analysis, the clinician tests multiple possible reinforcers at the same time within a single test condition.
The clinician first gathers information from caregivers and observations to identify situations in which challenging behavior typically occurs. Around 2014, Dr. Greg Hanley adapted the synthesized analysis to create the interview-informed synthesized contingency analysis (IISCA). In the IISCA format, the clinician conducts open-ended interviews with caregivers, then directly observes the behavior to identify information about it, such as triggers and precursors.
Heath says he turns to the IISCA when he needs to run a functional analysis. For him, one of the major benefits is that the IISCA allows practitioners to test multiple functions simultaneously.
“The traditional FA model isolates a single function,” Heath says, “whereas the IISCA synthesizes multiple variables to understand how they work together, which is more reflective of how behavior plays out in the real world.”
To test multiple functions simultaneously, the clinician runs a pairwise design with two alternating conditions: a test condition and a control condition. In the test condition, the clinician presents the combined situation (e.g., removing attention, adding demands, and restricting access to preferred items simultaneously). When the learner engages in the problem behavior, the clinician provides all relevant reinforcers together (such as attention, a break, and access to items). In the control condition, the clinician provides those outcomes freely and does not place demands.
Advantages:
- Efficient; identifies behavioral function quickly by testing multiple variables at once
- Reflects real-life situations more closely by combining triggers
- Practical; often easier for clinicians and caregivers to implement
Limitations:
- May produce inaccurate results because it combines multiple reinforcers in one condition
- Can identify functions that are not actually maintaining the behavior (false positives)
- May miss individual variables that influence behavior (false negatives)
- Interview can be biased
Example of an IISCA graph for ABA
How to conduct a traditional ABA functional analysis step-by-step
To conduct a traditional functional analysis, first set up a quiet, distraction-free space. Start with a control (play) condition where the learner has attention, preferred items, and no demands. Then test each condition by removing the relevant variable, like attention, items, or tasks. Collect response data across sessions and graph the results.
Here are the steps to run a traditional ABA functional analysis:
Graph and analyze the results
Graph the data with a multi-element design graph to visually compare patterns of responding across conditions. Identify which condition shows higher and consistent levels of behavior. Use this pattern to determine the likely function of the behavior and guide treatment planning.
Cheat sheet ABA functional analysis steps
Our free, one-page cheat sheet outlines the key steps of a functional analysis and serves as a practical guide for planning your next FA. Download it to stay organized, follow each step with confidence, and run an effective FA.

Download our cheat sheet to guide your next FA
Performing ABA functional analysis
Example scenarios of how ABA functional analysis works
These real-life example scenarios show how clinicians and researchers use functional analysis to identify what maintains problem behavior and guide intervention. Whether you use a traditional FA or another model, the results help clarify behavior function and support treatment plans that teach alternative behaviors that serve the same purpose.
Here are three example scenarios that show how functional analysis works in real life:
[fs-toc-omit]How to track results of ABA functional analysis
Clinicians track results of a functional analysis using a multi-element graph. This graph plots the behavior data that you take during each session and shows how often behavior occurs in each session. It allows you to compare patterns and identify which condition maintains the behavior.
In a multi-element functional analysis graph, each condition appears as its own data path. As you run sessions and add data points, the paths begin to separate. When one condition shows consistently higher levels of behavior than others, it suggests that condition maintains the behavior.
Here are the steps to track results of an ABA functional analysis using our multi-element graphing tool:
- Use our tracking sheet (below) to organize and collect data during each session
Use our free functional analysis multi-element graph template to record key data on each session. - Plot data on a multi-element graph
Graph each session as a data point. Use a different symbol or line for each condition (e.g., attention, escape, tangible, play). - Label conditions clearly
Make sure each data path is easy to identify so you can compare conditions at a glance. - Look for diverging data paths
As you continue to record data across sessions, look for one condition where behavior is consistently higher or lower than the others. - Identify the likely function
If behavior is highest in one condition and lower in others, that condition likely represents the function (e.g., escape, attention, access to items). - Check for consistency across sessions
Confirm that the pattern repeats across multiple sessions before making conclusions.
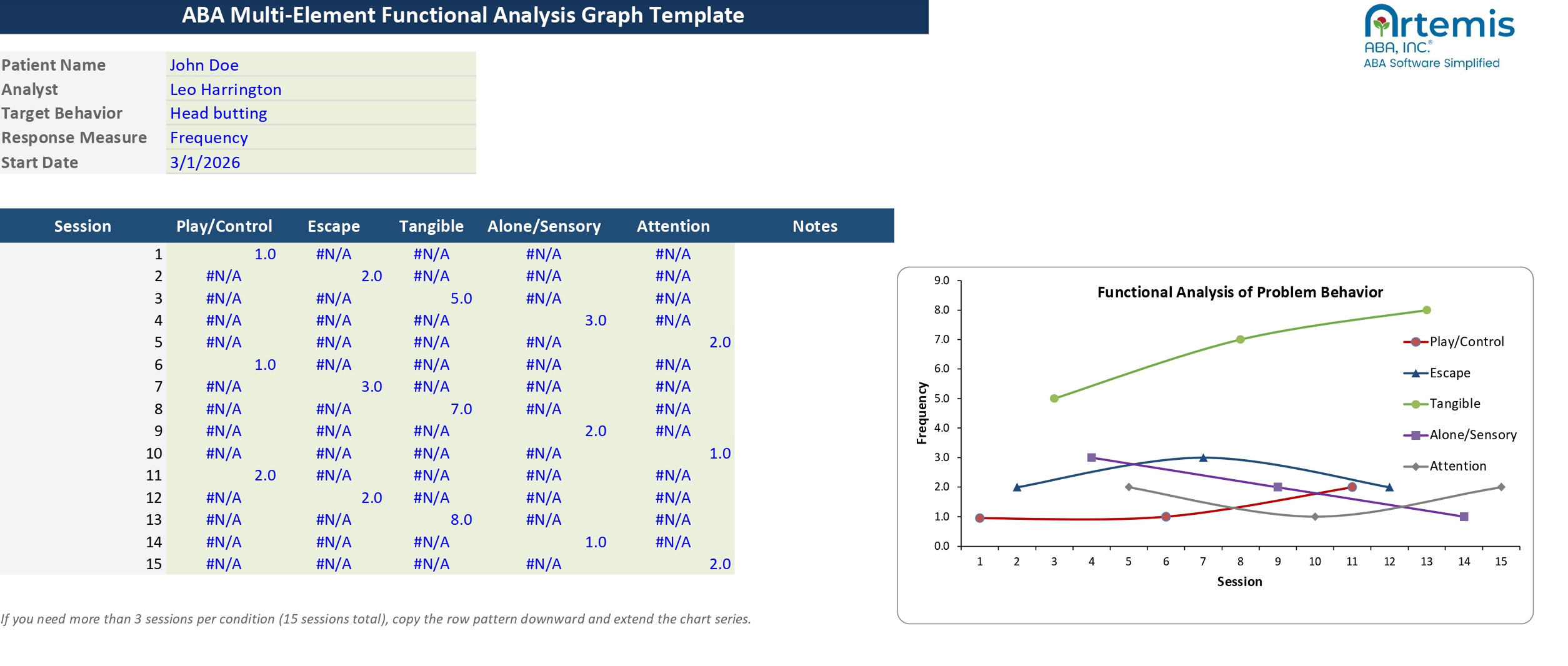
Multi-element design graph template for ABA functional analysis
Use our free multi-element functional analysis template to learn how to create and analyze a multi-element graph. The download includes a completed example so you can see what a finished graph looks like, along with a fill-in template that automatically updates as you enter data. Use it to visualize FA results, interpret patterns across conditions, and guide treatment planning.
Download our template and start visualizing your data today
[fs-toc-omit]How to evaluate an ABA functional analysis multi-element graph
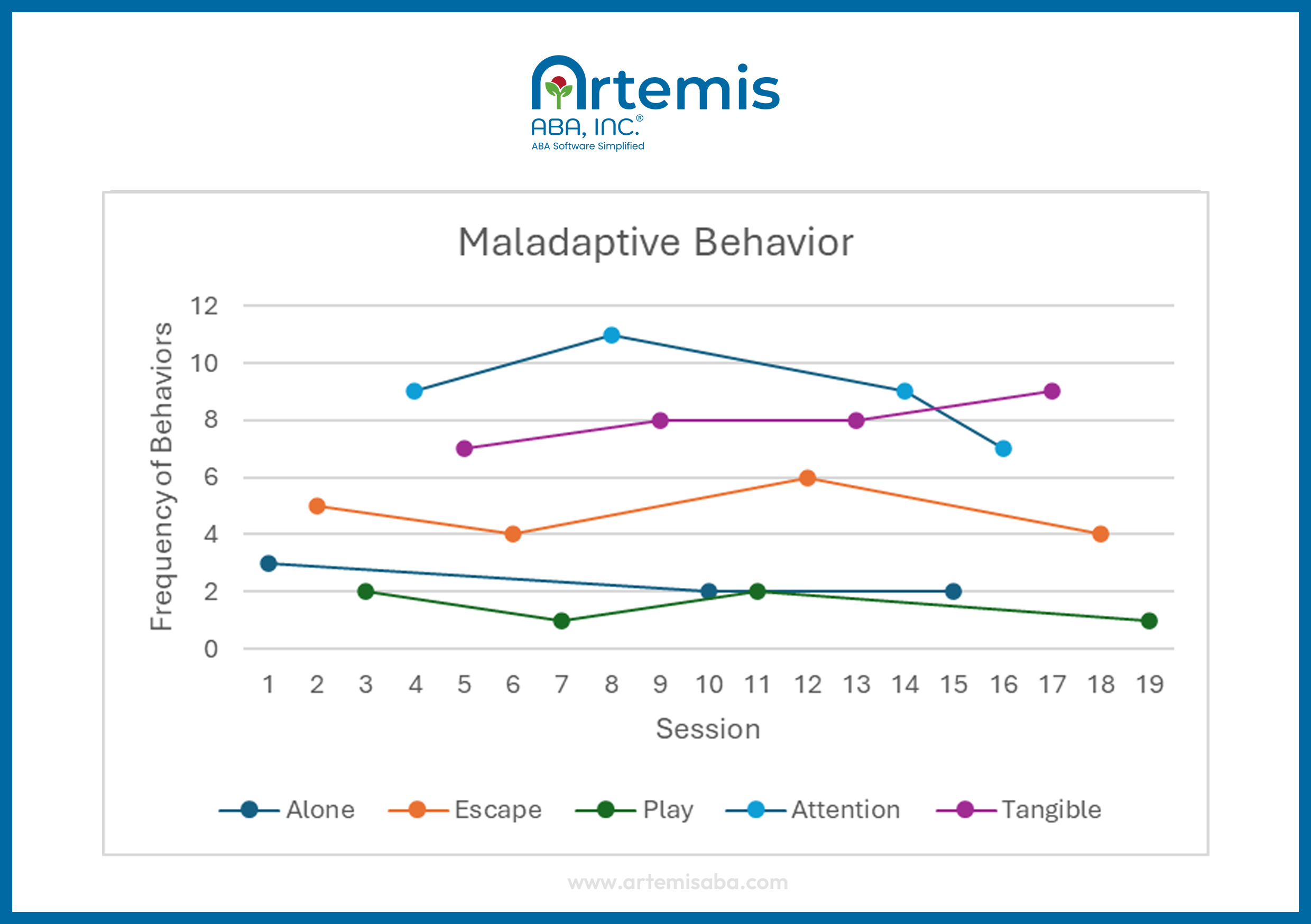
A multi-element graph shows how the learner’s behavior changes across conditions. Each data path shows the level of behavior during a specific condition. Compare the paths to identify any condition where behavior is consistently more frequent, which suggests that condition maintains the behavior.
In the graph below, the behavior appears to occur most often during the tangible condition, where the clinician provided access to preferred items after the problem behavior, then took them away to see if the learner would engage in the behavior again. This higher and more consistent level of responding suggests that access to tangibles is likely maintaining the behavior. In contrast, lower levels in other conditions help confirm that these functions are not maintaining the behavior as strongly.
Assessing an FA multi-element graph
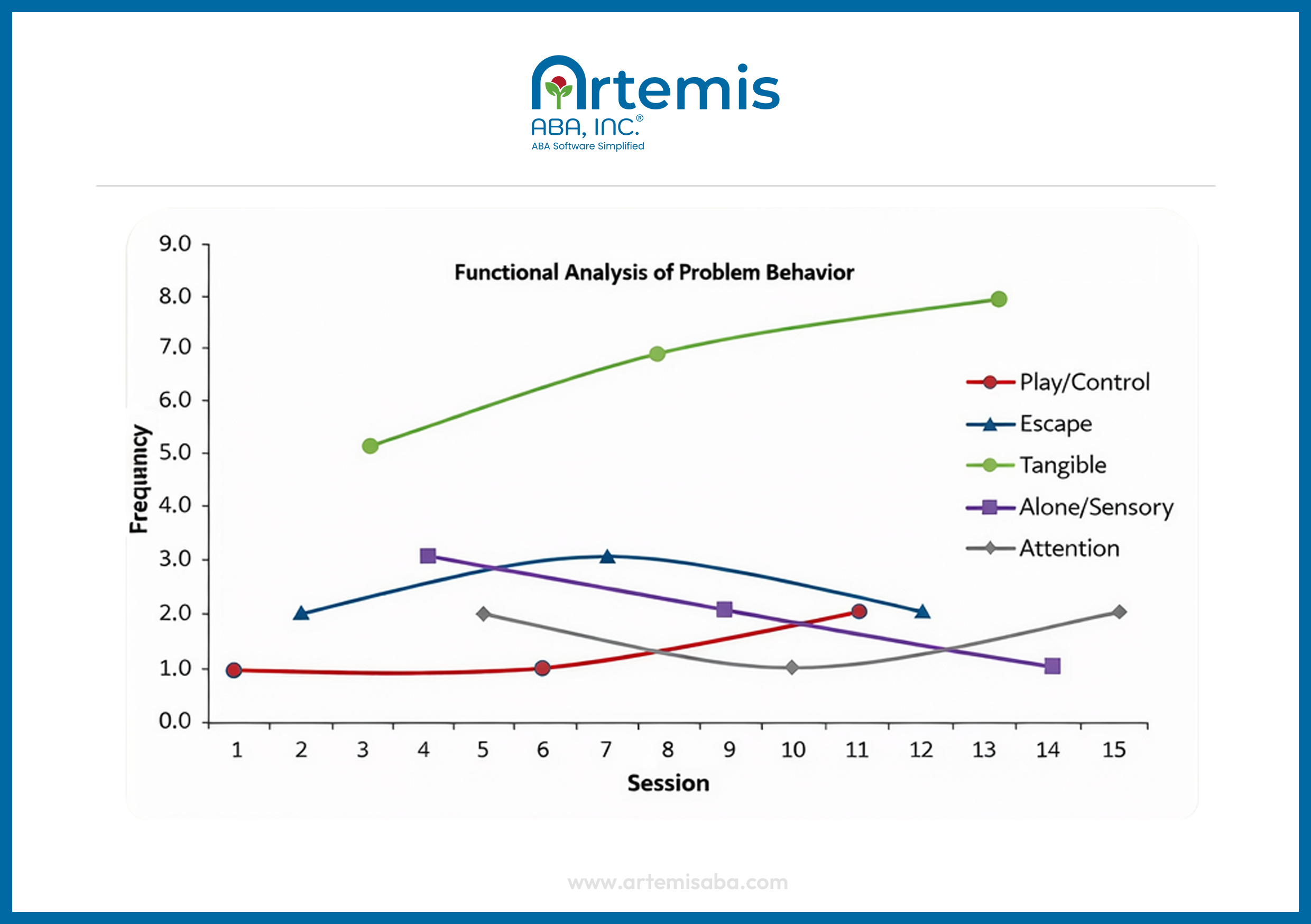
- Identify the data path with the highest level of responding – primary function (tangible)
- Compare to other conditions – rule out alternative functions
- Check control condition – verify low responding in absence of reinforcement
- Conclude that access to tangibles is reinforcing the problem behavior
[fs-toc-omit]Best practices for using functional analysis in your ABA practice
Best practices for using ABA functional analysis include starting with indirect and descriptive assessments before running an FA. Involve caregivers early and get consent. Have another clinician present. Use ABA software to track data so you can focus on observing behavior and running a safe, smooth analysis.
Here’s what ABA experts and professionals highlight as key best practices – the “do’s and don’ts” – for using functional analysis in your ABA practice:
Streamline your functional analysis with Artemis ABA
Artemis ABA is the software upgrade for clinics that want stronger data collection and analysis, including functional analysis. Artemis handles the busywork so clinicians can focus on clear assessments, effective interventions, and the work that drives real progress.
Artemis ABA connects data collection, analysis, scheduling, billing, and reporting into a single, all-in-one ABA practice management system. Its mobile-friendly tools and real-time data tracking allow clinicians to capture session data and monitor progress without interrupting therapy, while automated workflows reduce administrative burden and errors.
For functional analysis, features like real-time data visualization, centralized dashboards, and automated reporting make it easier to compare conditions, identify behavior patterns, and make faster, data-driven decisions. By replacing manual spreadsheets with a secure, cloud-based system, ABA clinics can outsource tedious tasks, gain data-driven insights to inform behavior interventions and spend more time with learners – the work that drives real progress.
Schedule Your Walkthrough

FAQ on ABA functional analysis
Is a functional analysis always necessary in ABA?

No, a functional analysis is not always necessary to determine the function of a behavior. Many ABA professionals use interviews and direct observation instead. Experts suggest using a functional analysis only when these simpler methods do not give a clear answer.
Who is qualified to conduct an ABA functional analysis?
BCBAs and other trained ABA professionals can run a functional analysis. Before you begin, review your training to ensure you use sound methods and collect accurate data.
What happens if the target behavior in a functional analysis is dangerous?
If the target behavior is dangerous, put safety measures in place before you start the functional analysis, such as protective equipment, and make sure you have staff who can intervene if necessary. Set clear rules for when to stop so the behavior does not get worse. Try to find the function with simpler, less invasive methods first.
What type of environment should ABA functional analysis be conducted in?
Use a controlled environment with as few distractions as possible. Clear the room of unnecessary furniture and remove items that may distract the learner. Choose a quiet space, and limit outside noise and visuals as much as possible.
Monday to Friday, 7 AM – 7 PM CST.
If you're reaching out outside these hours, please submit a support ticket—our team will respond as soon as possible.



%201.webp)


